
Diagnostic Value of Colour Doppler Twinkling Artefact in Detecting Nephrolithiasis
ORIGINAL ARTICLE
Diagnostic Value of Colour Doppler Twinkling Artefact in Detecting Nephrolithiasis
XJ Din, EY Hing, H Abdul Hamid
Department of Radiology, Faculty of Medicine, Universiti Kebangsaan Malaysia Medical Centre, Kuala Lumpur, Malaysia
Correspondence: Dr XJ Din, Department of Radiology, Faculty of Medicine, Universiti Kebangsaan Malaysia Medical Centre, Kuala
Lumpur, Malaysia. Email: xjdin@yahoo.com
Submitted: 7 Nov 2018; Accepted: 7 Jan 2019.
Contributors: All authors contributed to the concept or design, acquisition of data, analysis or interpretation of data, drafting of the manuscript,
and critical revision of the manuscript for important intellectual content of this study. All authors had full access to the data, contributed to the
study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of Interest: The authors have no conflict of interest to disclose.
Funding/Support: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics Approval: Ethical approval was granted by the Universiti Kebangsaan Malaysia Medical Centre Ethics Committee (Ref FF-2016-062).
Written informed consent was obtained from all participants on the day of examination.
Acknowledgement: The authors would like to express their gratitude to all the radiologists and radiographers in the Radiology Department as
well as the statistician for their contributions to this study.
Abstract
Objectives
To determine the sensitivity and specificity of adding colour Doppler ultrasonography, which demonstrates
twinkling artefact in the presence of stones, to B-mode ultrasonography in the detection of nephrolithiasis.
Methods
This was a cross-sectional prospective study conducted in the Radiology Department from June 2016 to
July 2017. Colour Doppler ultrasonography twinkling artefact assessment in addition to the conventional B-mode
ultrasonography was performed on patients who were being investigated for nephrolithiasis with unenhanced
computed tomography (CT). CT images were then correlated with sonographic findings. With CT as reference
standard, the sensitivity and specificity of adding colour Doppler to B-mode ultrasonography were calculated.
Results
A total of 121 calculi were detected with CT in 47 of our 57 patients. Sensitivity of B-mode ultrasonography
was 34.7% compared with 42.1% when additional colour Doppler ultrasonography was performed. The specificity
was 72.2% and 62.9% respectively. Sensitivity and specificity differences of these two imaging approaches are
statistically significant. Based on the size of the renal calculi, detection rate with merely B-mode ultrasonography
alone was 18.8% for calculi <5 mm, 50.5% for calculi 5-9 mm, 100% for calculi 10-19 mm and 90.9% for calculi
of ≥20 mm in measurement. The combined B-mode and colour Doppler ultrasonography had a corresponding
sensitivity of 23.5%, 72.2%, 100% and 100%.
Conclusion
The use of colour Doppler in addition to the conventional B-mode ultrasonography slightly increases
the sensitivity of nephrolithiasis detection with comparable specificity empirically. Although the overall sensitivity
and specificity of ultrasonography are rather low, it remains as an important screening tool for renal calculus due
to its availability, lower cost, non-invasive nature, and lack of ionising radiation.
Key Words: Calculi; Nephrolithiasis
中文摘要
彩色多普勒超聲閃爍偽影對檢測腎結石的診斷價值
XJ Din, EY Hing, H Abdul Hamid
目的
檢視彩色多普勒超聲閃爍偽影添加到B超對檢測腎結石的敏感性和特異性。
方法
這項橫斷面前瞻性研究於2016年6月至2017年7月期間在我院的放射科進行。對平掃CT尿路成像診斷的腎結石患者作常規B超檢查外添加彩色多普勒超聲閃爍偽影評估。然後將CT圖像與超聲檢查結果相關聯。以CT為參考標準下,檢視將彩色多普勒超聲閃爍偽影添加到B超的敏感性和特異
性。
結果
57名患者中,47例透過CT檢測共121粒結石。B超的敏感性為34.7%,添加彩色多普勒超聲閃
爍偽影後的敏感性為42.1%;特異性分別為72.2%和62.9%。兩種檢查方法的敏感性及特異性均有明
顯差異。單以B超檢查發現小於5毫米腎結石的檢出率為18.8%、5-9毫米腎結石50.5%、10-19毫米腎
結石100%,20毫米或以上腎結石90.9%。結合B超和彩色多普勒超聲的相應敏感性為23.5%、72.2%、
100%和100%。
結論
與常規B超檢查比較,結合彩色多普勒閃爍偽影檢查能稍微提高檢測腎結石的敏感度,特異
性於實證上則相若。儘管超聲檢查的總體敏感性和特異性較低,但由於它的可用性、較低成本、非
侵入性以及非電離輻射性質,它仍然是腎結石的重要篩查工具。
INTRODUCTION
Nephrolithiasis is a common condition in which
calculi are formed in the kidneys. The epidemiology of
nephrolithiasis differs according to geographical area
in terms of prevalence and incidence, age and gender
distribution, stone composition and stone location. Race,
diet, socio-economic status and climate are thought to be
the contributing factors of such differences.[1] The global
prevalence of the condition has increased from 3.25% in
the 1980s to 5.64% in the 1990s.[2] It has been predicted
that its prevalence among people residing in susceptible
regions would further increase from 40% in 2000 to 56%
by 2050.[2]
The main diagnostic modalities used for detection of
urinary tract calculi include ultrasonography and non-contrast
computed tomography (CT) of kidneys, ureters
and bladder. Although CT has been shown to be highly
sensitive (94%-100%) and specific (92%-100%), it
involves radiation exposure.[3] Therefore, ultrasonography
has been established as a screening tool in the early
detection of renal calculi as it is readily available,
inexpensive, and does not emit radiation.[4] However, the
detection rate reduces when a calculus is smaller than
3 mm in size or when a stone is located within a nondilated
pelvicalyceal system, thus jeopardising its
reliability as a useful diagnostic device.[5]
The twinkling artefact, or colour comet tail artefact,
is a colour Doppler phenomenon that appears as a
rapid interchange of colour behind a static object.[6] [7]
This artefact may also be demonstrated during power
Doppler and spectral Doppler scans, giving rise to
appearance of seemingly random vertical lines that form
a heterogeneous spectral expansion.[6]
The twinkling artefact is believed to be a form of intrinsic
noise fluctuation within the Doppler circuitry of the
ultrasonography equipment.[6] [8] Another theory suggests
that this artefact is created by a strongly reflecting
medium with a coarse and irregular surface, causing
numerous internal reflections in the medium, resulting
in prolonged pulse duration of the transmitted sound
signal.[7]
The detection of certain medical conditions such as
nephrolithiasis, nephrocalcinosis, calcified renal lesions
and vascular calcifications has shown promising outcome
with the application of this scintillation phenomenon.[6]
Its presence in the setting of urinary tract calculi is
associated with an improved contrast-to-noise ratio
when compared with posterior acoustic shadowing.[9]
The twinkle sign appears to be unaffected by frequency
of the ultrasound beam.[9] It is, however dependent on
several machine settings, which include location of the focal zone, colour filter, grey-scale gain, colour-white
priority, and pulse repetition frequency (PRF).[10] [11] It is
possible that this phenomenon can be utilised to improve
the sensitivity and specificity of ultrasonography in the
diagnosis of nephrolithiasis.
This prospective study was designed to evaluate
the benefit of adding colour Doppler to B-mode
ultrasonography in the detection of nephrolithiasis,
using CT as the reference standard. It was hoped that the
improvement in the detection of urolithiasis can obviate
the need for CT in some patients, thus reducing radiation
dose and the expenses involved in investigation.
METHODS
This was a cross-sectional prospective study conducted
in the Radiology Department from June 2016 to July
2017. Inclusion criteria were patients who presented with
symptoms such as colicky loin pain, recurrent urinary
tract infections, or haematuria, who were subsequently
investigated for nephrolithiasis with CT as requested
by clinicians, when colour Doppler ultrasonography
was performed in addition to the conventional B-mode
ultrasonography. Exclusion criteria included patients
who were incapable of giving consent, patients who
were critically ill, and those who were deemed unfit
to undergo ultrasonography. Patients with known
nephrocalcinosis and those who had >10 calculi on CT
were also excluded.
CT was performed with Siemens CT Somatom-64 in
which participants were required to have a full bladder
prior to the scheduled examination. The scan was then
performed with the patient positioned supine on the
gantry, scanning from the upper abdomen to symphysis
pubis. Parameters set for this examination include 5-mm
collimation, 120 kV, 200 mAs and reconstruction at 3-mm
intervals. Oral, intravenous, or rectal contrast were not
administered.
Sonographic examination was done on the same day
as CT for each patient by a registrar who has 3-year
radiology experience, using multiple new generation
ultrasound scanners (Toshiba TUS-X200 and Philips
HD11 XE) with curved-phase array transducers. The
examiner was blinded to the findings of CT scan. Grey-scale
ultrasonography was first carried out to detect
any abnormal foci of renal echogenicity with posterior
acoustic shadowing. Emphasis was given on the site
and size of these abnormalities. Subsequently, colour
Doppler ultrasonography was performed by applying the colour window onto the area(s) of interest and adjacent
tissue, with the PRF set just above the threshold for
colour mapping of the renal vessels (>60 cm/s). The
operator then assessed for a twinkling artefact with
attention given to the location of the abnormal signal
and whether it was associated with the presence of renal
echogenicity or posterior shadowing.
CT images were reviewed by two observers (radiologists)
separately. In cases of disagreement, a consensus
agreement on the radiological findings was reached.
Sonographic findings were then correlated with CT,
which was used as the gold standard. The sensitivity
and specificity of adding colour Doppler to B-mode
ultrasonography were calculated.
RESULTS
A total of 70 individuals were enrolled in the study.
Thirteen of them with >10 calculi and nephrocalcinosis
were excluded. The final patient cohort consisted of
57 patients (31 males and 26 females). Their age ranged
between 25 and 78 years, with a mean of 55.3 years.
Ethnically, there were 45 (78.9%) Malay, nine (15.8%)
Chinese and three (5.3%) Indian patients.
Out of the 57 patients, 121 stones were detected
in 47 of them on non-contrast CT. Nephrolithiasis
was correctly diagnosed in 29 patients (61.7%) with
conventional B-mode ultrasonography and 31 patients
(66%) with the application of both B-mode and Doppler
ultrasonography. Using only grey-scale ultrasonography,
the sensitivity of calculus detection was 34.7%
(42 calculi) with 72.2% specificity. The sensitivity
increased to 42.1% (51 calculi) by using both B-mode
and Doppler ultrasonography, with specificity of 62.9%
(Table 1). Figures 1 and 2 show twinkling artefacts with
calculi measuring 8 mm and 3 mm, respectively.
Table 1. Diagnostic indices of nephrolithiasis, using only
conventional grey-scale ultrasonography and grey-scale
plus colour Doppler ultrasonography with twinkling artefact
assessment.
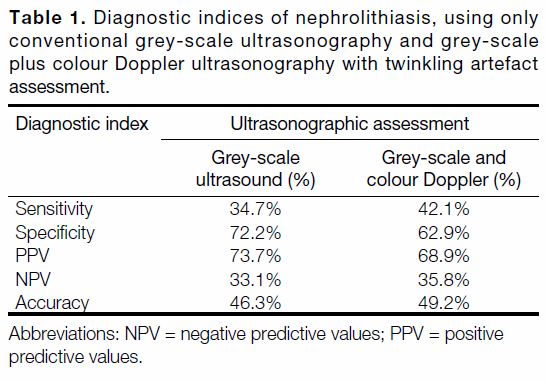
Figure 1. A 66-year-old woman with left flank pain. (a) Ultrasonograph showing echogenic focus (8 mm) with posterior acoustic shadowing
(arrow) in the left kidney. (b) Colour Doppler ultrasonograph showing corresponding twinkling artefact (arrow). (c) Diagnosis of left
nephrolithiasis was confirmed by computed tomography (arrow).
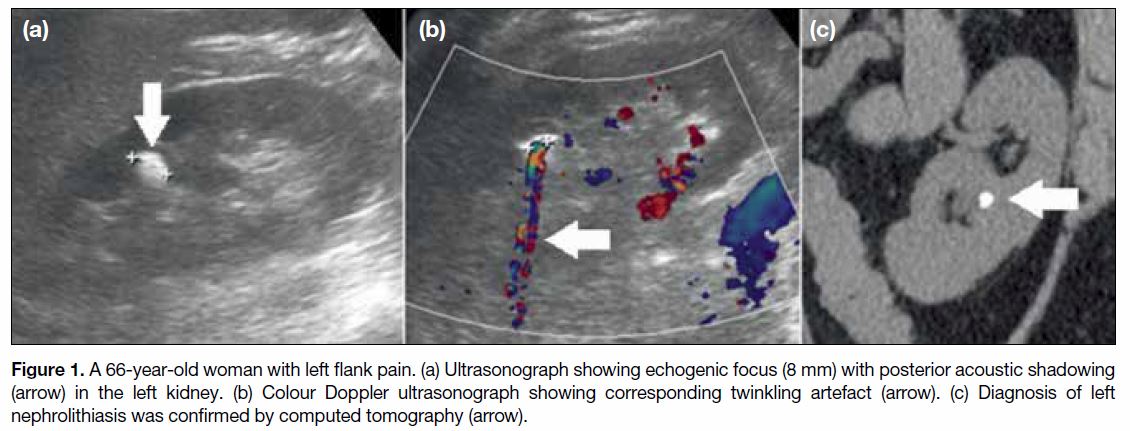
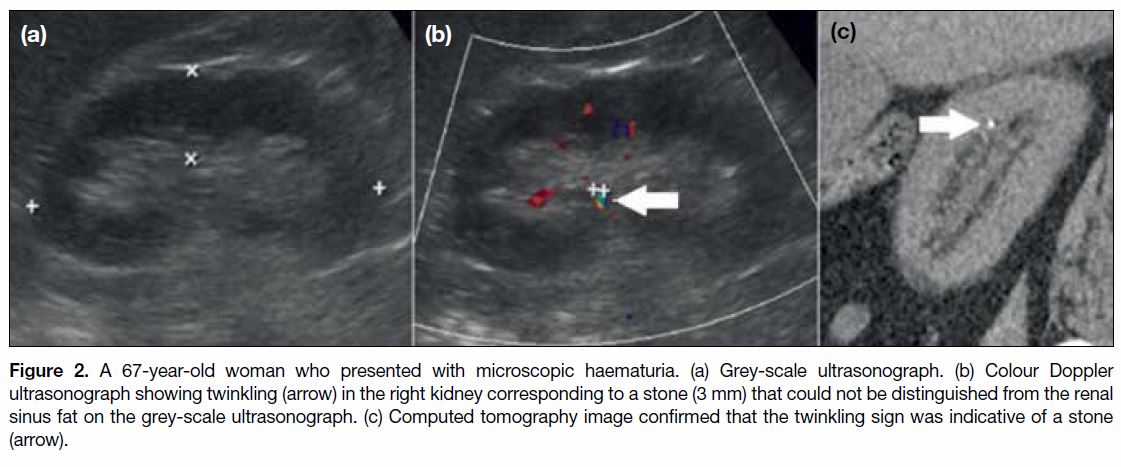
Figure 2. A 67-year-old woman who presented with microscopic haematuria. (a) Grey-scale ultrasonograph. (b) Colour Doppler
ultrasonograph showing twinkling (arrow) in the right kidney corresponding to a stone (3 mm) that could not be distinguished from the renal
sinus fat on the grey-scale ultrasonograph. (c) Computed tomography image confirmed that the twinkling sign was indicative of a stone
(arrow).
The detection rate of nephrolithiasis varied based
on size of the calculus. With conventional B-mode
sonography alone, sensitivity of detection was 18.8%
for calculi of 1-4 mm, 50.5% for calculi of 5-9 mm,
100% for calculi of 10-19 mm and 90.9% for calculi
of ≥20 mm in diameter. The corresponding specificity
was 91%, 39.1%, 100% and 100% (Table 2).
Table 2. Sensitivity and specificity of grey-scale ultrasonography
and grey-scale plus colour Doppler ultrasonography with twinkling
artefact assessment, based on the size of the renal calculi.
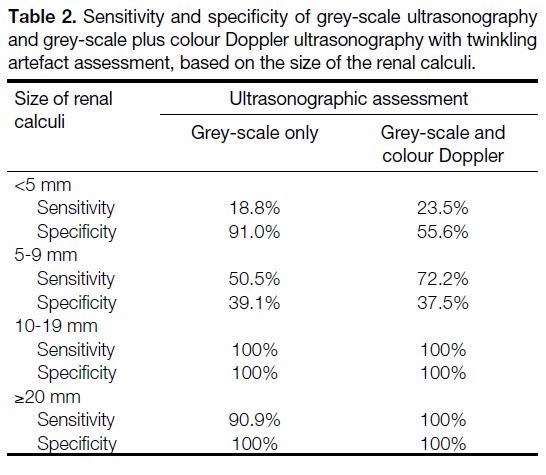
When complimentary colour Doppler was added to
the examination, 23.5% of 1-4 mm calculi, 72.2% of
5-9 mm calculi, 100% of 10-19 mm calculi and 100%
of calculi ≥20 mm in size were detected. The specificity
was 55.6%, 37.5%, 100% and 100%, respectively
(Table 2).
DISCUSSION
Non-contrast spiral CT remains the gold standard for
diagnosing urinary calculi with promising sensitivity
and specificity.[3] [12] Nevertheless, exposure to ionising
radiation following a CT examination is one of the
main limiting factors of its clinical implementation,
especially when children and young adults are involved.[8]
Thus, ultrasonography, which is more readily available,
inexpensive, and devoid of ionising radiation,[4] became
another convenient alternative.
Literature on ultrasonography as a diagnostic tool for
renal calculi is diverse. Vijayakumar et al[5] stated that
complementing standard grey-scale sonogram with
twinkling artefact assessment improves detection of
urolithiasis. Likewise, Lee et al[13] reported that comet-tail
artefact on colour Doppler had a sensitivity of 75%
for calculi between 5 mm and 9 mm and 100% for
stone <5 mm or >10 mm. Kielar et al[14] noticed that by
adding Doppler evaluation, the sensitivity and positive
predictive value for stones ranging from 1 mm to 9 mm
in size improved from 80.2% to 83% and 64.9% to 94%,
respectively. In a study by Shabana et al,[9] the twinkling
sign increased the contrast-to-noise ratio when compared
with posterior acoustic shadowing. Turrin et al[15]
concluded that patients with urinary calculi are more
likely to have twinkling phenomenon on their colour
Doppler ultrasonography (95.5%) than were those
without urinary calculi (9.0%). Studies by Korkmaz et al,[16]
Yavuz et al,[17] and Aytaç and Ozcan[18] found that the
Doppler phenomenon produced satisfactory results in
detecting small calculi (≤5 mm), especially in the setting
of equivocal findings on B-mode scanning.
The pattern of our results is similar to outcomes of
the abovementioned studies, where the sensitivity
was slightly higher when both B-mode and Doppler
techniques were utilised together (42.1%), compared
with sole grey-scale scanning (34.7%).
Ultrasonography gives a wide range of sensitivities in
different studies, due to patient population, body habitus,
technical variations, reference standards, location,
and size of the calculus.[19] The overall detection rates
in our study were low for both grey-scale and colour
Doppler ultrasonography. This could be partly due
to the larger numbers of calculi present in the studied
population, where 121 calculi were found in 47 of our
57 participants (2.6 calculi/patient). A prospective
study by Ahmad and Abdallah7 concluded that
sonographic examination with adjunct colour Doppler ultrasonography has a higher sensitivity (68%) in
detecting urinary calculi than does posterior acoustic
shadowing (62%) or echogenic focus on greyscale
(58%); however, those authors found only 100 calculi
in a sample size of 71 patients (1.4 calculi/person).
A similar study design by Dillman et al[8] with sample
cohort of 49 and confirmed urinary calculi of 132 from
CT (2.7 calculi/person), came to a conclusion that
twinkling artefact is relatively insensitive (55%)
in routine practice with a high false-positive rate
(51%). It could be technically challenging to identify
and segregate each calculus with ultrasonography,
especially when they are small and close to one another.
Other studies with similar results include Ulusan et al[20] and
Fowler et al,[21] who considered ultrasonography a limited
tool in the detection of nephrolithiasis. Sorensen et al[22]
reported that B-mode is more sensitive than colour
Doppler ultrasonography when each of them is applied
separately. Hence, colour Doppler ultrasonography
should always be viewed as an extra tool to enhance
grey-scale ultrasonographic findings, rather than as an
isolated assessment.
According to Brisbane et al,[19] calculi of <3 mm may
not produce acoustic shadowing and thus could be
frequently missed on ultrasonography. In our study, the
incidence of correctly identifying a stone decreased with
decreasing calculus size. The sensitivity of identifying a
calculus <5 mm was 18.8% with grey-scale and 23.5%
with both techniques.
The specificities of calculus detection with grey-scale
sonography as well as the combined grey-scale and
colour Doppler methods were comparable (72.2% and
62.9% respectively). As our patients were all referred for
radiological assessment owing to clinical suspicion of
nephrolithiasis, there were only 10 (17.5%) of 57 patients
in whom no renal calculi were identified. Selection bias
with an insufficient control population may be one of the
causes of its low specificity.
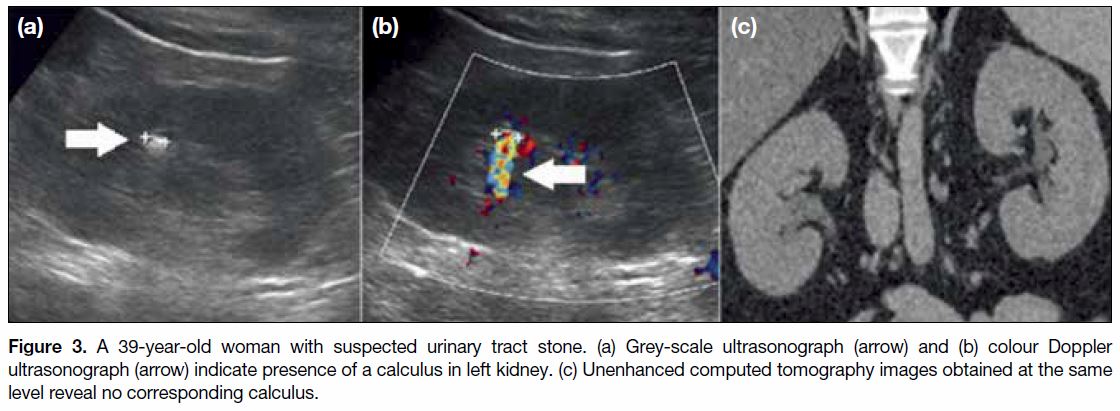
When colour Doppler ultrasonography is applied, renal
vascularity and high attenuating conditions such as
medullary calcinosis, vascular calcification, surgical
clips, and stents may sometimes mimic the appearance
of twinkling artefact, as seen in Figure 3. Therefore, a
slightly higher false positive value was seen with the
combined technique (n = 18) as opposed to grey-scale
ultrasonography alone (n = 16). A 51% false-positive
rate was recorded by Dillman et al.[8]
Figure 3. A 39-year-old woman with suspected urinary tract stone. (a) Grey-scale ultrasonograph (arrow) and (b) colour Doppler
ultrasonograph (arrow) indicate presence of a calculus in left kidney. (c) Unenhanced computed tomography images obtained at the same
level reveal no corresponding calculus.
Our study has several limitations. First, it had a relatively
small sample size of 57 patients. Second, two different
models of ultrasound machines were used for the study.
Although the PRF was adjusted for each patient to
the recommended threshold, the intrinsic setting and
performance of each machine may still differ from each
another and thus interfere with the interpretation and end
results.[10] [11]
Apart from renal vascularity, the presence of high
attenuating structures and machine settings, other
factors which influence the intensity and appearance
of twinkling effect include motion, surface roughness,
and components of the calculus.[10] As genetic and
environmental factors such as dietary practices and
regional climate may affect the prevalence of stone
disease,[2] data collected from our centre might not
mimic the results of studies conducted in other regions.
Another purported pitfall of ultrasonography is its lack
of reliability in detecting ureteric calculi.[14] The overlying
bowel gas hinders the usefulness of sonography, affecting
twinkling assessment to an even greater extent.
For further strengthening of this research, a study with a
larger sample size and longer duration may be necessary.
Proper optimisation of ultrasound machines in terms of
its gain, depth and alternate modes (such as flash and
stone modes) may enhance the process of data collection
and thus obtaining a larger patient cohort.[5]
Regardless of the low sensitivity of ultrasonography in
the detection of urinary calculi, adding colour Doppler
ultrasonography can improve its sensitivity compared
with grey-scale alone. This would increase clinicians’ diagnostic confidence in the diagnosis of small stones,
especially in patients with symptoms of nephrolithiasis
who do not require CT or surgical intervention.
Nonetheless, radiologists should be acquainted with
the higher false-positive ratio when both techniques are
employed simultaneously.
CONCLUSION
The use of colour Doppler ultrasonography in addition
to the conventional B-mode ultrasonography slightly
increases the sensitivity of nephrolithiasis detection
with comparable specificity. Even though the overall
sensitivity and specificity of ultrasonography are rather
low, it remains as an important screening tool for renal
calculi due to its availability, lower cost, non-invasive
nature and lack of ionising radiation.
REFERENCES
1. Trinchieri A. Epidemiology of urolithiasis: An update. Clin Cases
Miner Bone Metab. 2008;5:101-6.
2. Romero V, Akpinar H, Assimos DG. Kidney stones: a global
picture of prevalence, incidence and associated risk factors. Rev
Urol. 2010;12:e86-96.
3. Türk C, Petřík A, Sarica K, Seitz C, Skolarikos A, Straub M, et al.
EAU guidelines on diagnosis and conservative management of
urolithiasis. Eur Urol. 2016;69:468-74. Crossref
4. Patlas M, Farkas A, Fisher D, Zaghal I, Hadas-Halpern I. Ultrasound
vs. CT for the detection of ureteric stones in patients with renal
colic. Br J Radiol. 2001;74:901-4. Crossref
5. Vijayakumar M, Ganpule A, Singh A, Sabnis R, Desai M. Review
of techniques for ultrasonic determination of kidney stone size. Res
Rep Urol. 2018;10:57-61. Crossref
6. Michael Hirsch S, Tamara Palavecino B, Boris León R. Color
Doppler twinkling artifact: A misunderstood and useful sign. Rev
Chil Radiol. 2011;17:82-4. Crossref
7. Ahmad SK, Abdallah MM. The diagnostic value of the twinkle
sign in color Doppler imaging of urinary stones. Egyptian J Radiol
Nucl Med. 2014;45:569-74. Crossref
8. Dillman JR, Kappil M, Weadock WJ, Rubin JM, Platt JF,
DiPietro MA, et al. Sonographic twinkling artifact for renal calculus
detection: correlation with CT. Radiology. 2011;259:911-6. Crossref
9. Shabana W, Bude RO, Rubin JM. Comparison between color
Doppler twinkling artifact and acoustic shadowing for renal calculus
detection: an in vitro study. Ultrasound Med Biol. 2009;35:339-50. Crossref
10. Kamaya A, Tuthill T, Rubin JM. Twinkling artifact on color
Doppler sonography: dependence on machine parameters and
underlying cause. AJR Am J Roentgenol. 2003;180:215-22. Crossref
11. Kim HC, Yang DM, Jin W, Ryu JK, Shin HC. Color Doppler
twinkling artifacts in various conditions during abdominal and
pelvic sonography. J Ultrasound Med. 2010;29:621-63. Crossref
12. Dubinsky TJ, Sadro CT. Acute onset flank pain—suspicion of stone
disease. Ultrasound Q. 2012;28:239-40. Crossref
13. Lee JY, Kim SH, Cho JY, Han D. Color and power Doppler
twinkling artifacts from urinary stones: clinical observations and
phantom studies. AJR Am J Roentgenol. 2001;176:1441-5. Crossref
14. Kielar AZ, Shabana W, Vakili M, Rubin J. Prospective evaluation
of Doppler sonography to detect the twinkling artifact versus
unenhanced computed tomography for identifying urinary tract
calculi. J Ultrasound Med. 2012;31:1619-25. Crossref
15. Turrin A, Minola P, Costa F, Cerati L, Andrulli S, Trinchieri A.
Diagnostic value of colour Doppler twinkling artefact in sites negative for stones on B mode renal sonography. Urol Res.
2007;35:313-7. Crossref
16. Korkmaz M, Aras B, Sanal B, Yücel M, Güneyli S, Koçak A,
et al. Investigating the clinical significance of twinkling artifacts
in patients with urolithiasis smaller than 5 mm. Jpn J Radiol.
2014;32:482-6. Crossref
17. Yavuz A, Ceken K, Alimoglu E, Kabaalioglu A. The reliability
of color Doppler “twinkling” artifact for diagnosing millimetrical
nephrolithiasis: comparison with B-Mode US and CT scanning
results. J Med Ultrason. 2015;42:215-22. Crossref
18. Aytaç SK, Ozcan H. Effect of colour Doppler system on the
twinkling sign associated with urinary tract calculi. J Clin
Ultrasound. 1997;27:433-9. Crossref
19. Brisbane W, Bailey MR, Sorensen MD. An overview of kidney
stone imaging techniques. Nat Rev Urol. 2016;13:654-62. Crossref
20. Ulusan S, Koc Z, Tokmak N. Accuracy of sonography for detecting
renal stone: comparison with CT. J Clin Ultrasound. 2007;35:256-61. Crossref
21. Fowler KA, Locken JA, Duchesne JH, Williamson MR. US
for detecting renal calculi with nonenhanced CT as a reference
standard. Radiology. 2002;222:109-13. Crossref
22. Sorensen MD, Harper JD, Hsi RS, Shah AR, Dighe MK, Carter SJ,
et al. B-mode ultrasound versus color Doppler twinkling artifact in
detecting kidney stones. J Endourol 2013;27:149-53. Crossref
| Attachment | Size |
|---|---|
| v23n4_Diagnostic.pdf | 527.75 KB |