
Comparison of Vacuum Pressure Syringe Aspiration Technique with Penumbra Aspiration Thrombectomy System: an In Vitro Study
ORIGINAL ARTICLE
Comparison of Vacuum Pressure Syringe Aspiration Technique
with Penumbra Aspiration Thrombectomy System: an In Vitro Study
C Kobkitsuksakul1,2, T Jaroenngarmsamer2
1 Division of Interventional Neuroradiology, Department of Radiology, Ramathibodi Hospital, Mahidol
University, Bangkok, Thailand
2 Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Dr C Kobkitsuksakul, Division of Interventional Neuroradiology, Department of Radiology, Ramathibodi Hospital,
Mahidol University, Bangkok, Thailand. Email: dr.chai.kobkitsuksakul@gmail.com
Submitted: 2 Mar 2019; Accepted: 23 Apr 2019.
Contributors: Both authors contributed equally to the concept and design of the study, acquisition of the data, analysis and interpretation of the
data, drafting of the manuscript, and critical revision of the manuscript for important intellectual content. Both authors had full access to the data,
contributed to the study, approved the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of Interest: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Funding/Support: We thank Cultivating Medical-Scientific Expertise for Medical Students Program, Faculty of Medicine, Ramathibodi Hospital,
Mahidol University for support. We also thank the Research Center of Ramathibodi Hospital staff for providing equipment and experimental
space.
Ethics Approval: This study included no human or animal subjects; ethics approval was not required.
Declaration: We certify that this work was poster presented at the XXI Symposium Neuroradiologicum during 19-23 March 2018 at Taipei,
Taiwan, and no work resembling the enclosed article has been published or is being submitted for publication elsewhere.
Abstract
Objective
In aspiration thrombectomy, a 60-mL syringe has a higher aspiration force than a 20 inHg aspiration
pump. The recommended pressure of a new pump (Penumbra Pump MAX) is 28.5 inHg. We evaluated and compared
the negative pressure flow rates during aspiration from locked syringes to the Penumbra Pump MAX. We also sought
to determine how an increase in syringe volume affects the duration and volume of aspiration phases.
Methods
A Penumbra Pump MAX, a 60-mL VacLok negative pressure syringe, and a 100-mL syringe were used
as negative pressure generators and were connected to catheters. The pump was allowed to reach its peak negative
pressure at 28.5 inHg before aspiration. The 100-mL syringe was pulled to 60, 70, 80, and 90 mL and locked. The
mean flow rates (mL/s) and standard deviations were calculated.
Results
The 60-mL syringe created higher flow rates than the Penumbra Pump MAX at 28.0 inHg (5.51 vs.
5.01 mL/s). Every 10 mL increase in syringe volume extended the plateau phase by 2 s without altering the flow rate,
acceleration phase, or deceleration phase.
Conclusion
The aspiration power of the two negative pressure generators was comparable. Increasing syringe
volume directly increases the effective aspiration time.
Key Words: Hydrodynamics; Stroke; Suction; Syringes; Thrombectomy
中文摘要
真空壓力注射器抽吸技術與Penumbra抽吸血栓切除術的比較:體外研究
C Kobkitsuksakul、T Jaroenngarmsamer
目的
在抽吸血栓切除術中,60 mL注射器的抽吸力比20 inHg抽吸泵更高。新一代Penumbra Pump
MAX的建議壓力為28.5 inHg。本研究旨在評估和比較 Penumbra Pump MAX 和不同容量的鎖緊式注
射器在抽吸時的負壓流速,並檢視注射器容積增加時如何影響不同抽吸時相的持續時間和容積。
方法
將Penumbra Pump MAX、60-mL VacLok負壓注射器和100-mL注射器用作負壓發生器並將其
連接到導管上。抽吸前使泵達到其最大負壓的28.5 inHg。將100-mL注射器拉至並鎖定於60mL、
70mL、80mL和90 mL,計算其平均流速(mL / s)和標準差。
結果
:60-mL注射器在負壓為28.0 inHg時產生的流速(5.51 mL / s)高於Penumbra Pump MAX
(5.01 mL / s)。注射器容積每增加10 mL時流速平穩期可延長2秒而不改變整體流速、加速時段或減
速時段。
結論
兩種負壓發生器的抽吸力相若,增加注射器容積可增加有效抽吸時間。
INTRODUCTION
In the treatment of acute ischaemic stroke, syringes or an
aspiration pump are used as negative pressure generators.
They are used exclusively in aspiration thrombectomy,
in which the distal end of a large-bore catheter directly
aspirates a clot at large vessel occlusion sites.[1] [2] They
are used adjunctively in stent-retrieval thrombectomy
(Solumbra technique), which combines stent retrieval
with suction thrombectomy.[3] In both methods, the
choice of a negative pressure generator is up to the
interventionists, who take into consideration the pros and
cons of both devices, including aspiration power and, for
syringes, the size (20-60 mL).
A recent study showed that the aspiration power of a
60-mL locked syringe (a syringe pulled and locked at
60 mL in a closed system to create negative pressure)
was higher than the pressure of an aspiration pump
(20.0 inHg, recommended by the manufacturer). Even
though the pump could reach its highest negative
pressure at 26.5 inHg, the syringe force was still superior
to the pump.[4] A new device, the Penumbra Pump MAX
(Penumbra, Inc., Alameda [CA], US) has a recommended
pressure of 28.5 inHg, raising the question as to whether
the 60-mL syringe still has a higher aspiration force than
a 28.5-inHg aspiration pump.
A study by Simon and Grey[5] indicated that the dynamic
pressure and average flow rate of the Penumbra System pump were lower than all syringe sizes (3-60 mL). The
larger the syringe, the higher the static and dynamic
pressure attained. However, the pump had higher static
pressure than all syringe sizes.[5] This contradiction of
higher static pressure and lower dynamic pressure of the
pump compared with syringes led us to focus mainly
on the dynamic rather than the static characteristics of
aspiration. Moreover, a newer pump, the Penumbra
Pump MAX, with a higher adjusted pressure (28.5 inHg
vs. the studied pump 26.5 inHg) has been developed,
suggesting that a new comparison would be relevant.
The primary objective of this study was to evaluate and
compare the flow rates during aspiration created by
negative pressure from locked syringes to the Penumbra
Pump MAX, while the secondary objective was to
determine how a larger 100-mL syringe affects time and
volume of phases of the aspiration.
METHODS
A Penumbra Pump MAX, a 60-mL VacLok negative
pressure syringe (Merit Medical System Inc., South
Jordan [UT], US), and a 100-mL syringe (Wilburn
Medical, Kernersville [NC], US) locked by an external
device were used as negative pressure generators. The
Penumbra Pump MAX, together with a MAX Canister
and high-flow aspiration tubing, were connected to a
Penumbra ACE68 reperfusion catheter as per the standard
method. The pump was allowed 30 s to reach its peak negative gauge pressure of 28.5 inHg before aspiration
for 120 s. The aspiration characteristics were defined
as the acceleration phase at the beginning of aspiration;
followed by the plateau phase, where the aspiration rate
was constant; and ended with the deceleration phase.
Syringes were connected to a two-way valve before
connection to the ACE catheter. Since the largest volume
of a lockable syringe commercially available is 60 mL,
the 100-mL syringe was pulled to initial volumes of 60,
70, 80, and 90 mL and locked using two steel Vernier
callipers. Negative pressure was created before the valve
was opened until the flow rate reached the deceleration
phase and aspiration stopped. The experiment was set to
mimic free-flow aspiration using water as a medium. The
weight of water aspirated at the distal tip of the catheter
was recorded every 2 s by a two-digit digital analytical
balance device, and the mean flow rate (mL/s) was
calculated at the plateau phase for the syringes and at 2 s
to 120 s for the pump. The first 2 s were the acceleration
phase of all equipment and were excluded from the
calculation. Each experiment was repeated 10 times
(n = 10), and the mean flow rates (mL/s) and standard
deviations of the samples were calculated.
RESULTS
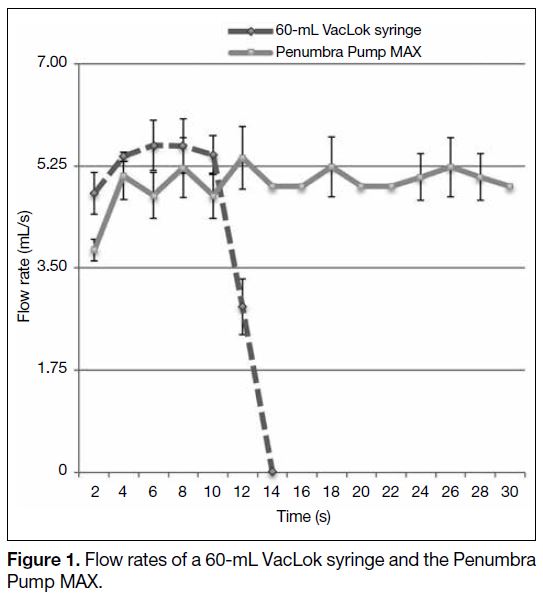
The Penumbra Pump MAX created a constant flow rate
without a plateau phase, while the 60-mL VacLok syringe
created higher flow rates than the Penumbra Pump MAX
(5.51 mL/s vs. 5.01 mL/s, p < 0.001) [Figure 1].
Figure 1. Flow rates of a 60-mL VacLok syringe and the Penumbra Pump MAX.
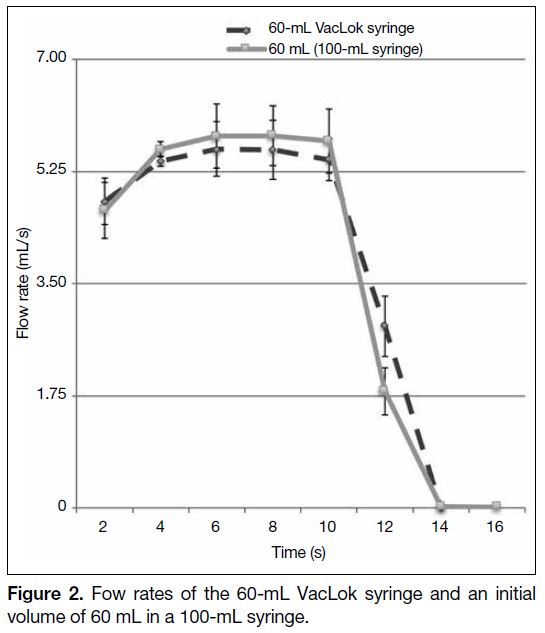
The hydrodynamic character of all syringes began with
an acceleration phase for 2 s, followed by a plateau
phase, and ended with a deceleration phase before
fluid filled the syringes. The 60-mL VacLok syringe
and the 60-mL initial volume of the 100-mL syringe
had the same 8-s plateau phase even though the latter
created a slightly higher average flow rate (5.51 mL/s vs.
5.73 mL/s, p < 0.001) [Figure 2].
Figure 2. Fow rates of the 60-mL VacLok syringe and an initial volume of 60 mL in a 100-mL syringe.
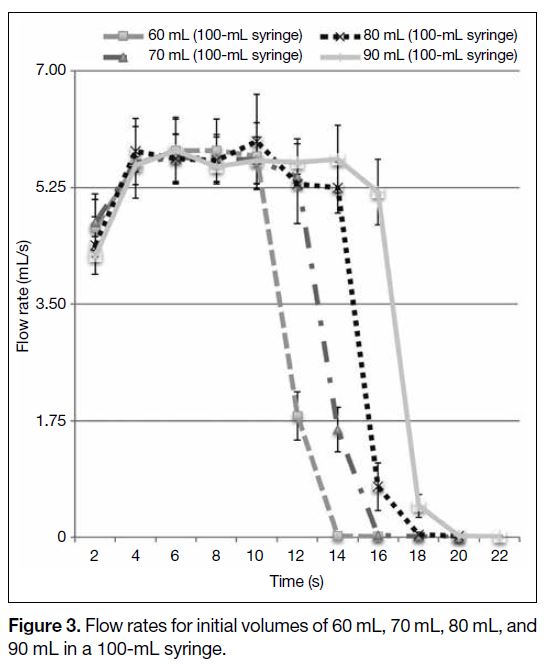
For the plateau phase of the 100-mL syringe, the larger
the initial volume, the longer the achieved plateau phase
was, that is, 10 s (70 mL), 12 s (80 mL), 14 s (90 mL)
[Figure 3]. Flow rates of all initial volumes were
comparable with one another.
Figure 3. Flow rates for initial volumes of 60 mL, 70 mL, 80 mL, and 90 mL in a 100-mL syringe.
DISCUSSION
Even though the 60-mL VacLok syringe generated a
higher flow rate than the Penumbra Pump MAX, the
syringe had a flow rate comparable with that of the
pump, which was tested by the company at 5.51 mL/s
versus 5.47 mL/s (unpublished data, 2017). This may be due to lower maximal negative pressure reached by the
pump in this experiment at 28 inHg, an acceptable range
for standard treatment, compared with the 28.5 inHg
reached by the company. This means the Penumbra
Pump MAX must always reach 28.5 inHg to achieve
equal aspiration power as a 60-mL VacLok syringe. The flow rates of this study were higher than previous results
due to a larger bore of ACE68 catheter (1.73 mm) versus
5MAX catheter (1.37 mm).[5]
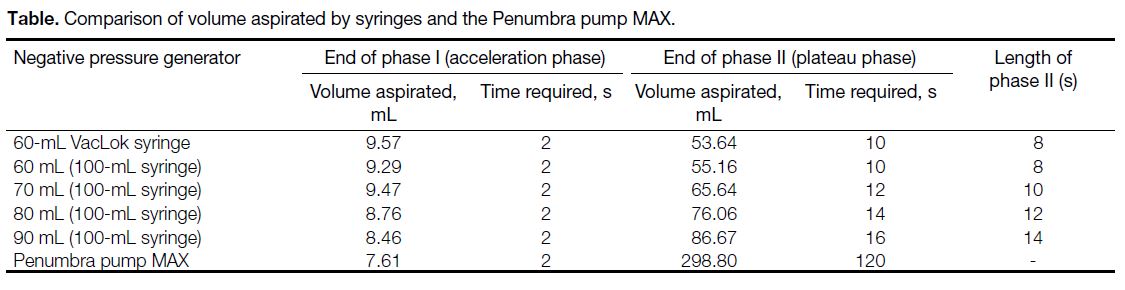
In practice, phases will be volume-dependent instead
of time-dependent (Table). Whenever the catheter
fully engages the clot, no flow enters the catheter and
the negative pressure will remain constant at that
volume-specific phase. The aspiration capability will be
extended, especially in blood with high viscosity. In the
partial flow condition, a 60-mL syringe could reach >60 s
of its plateau phase in a blood-like fluid as shown in a
previous study.[4] However, in the worst-case scenario of
dislodgement of a partial clot, the flow may enter a near
free-flow stage, and the syringe may not reach the stated time, <30 s in water aspiration. In contrast, an aspiration
pump is able to aspirate in a free-flow condition for >120 s,
outperforming the short plateau phase of the 60-mL
VacLok syringe and with no doubt the routinely used
20-mL and 50-mL syringes. With a limited plateau
phase, syringes cannot be used in the new CAPTIVE
technique,[6] which requires long aspiration times before,
during, and after stent retriever deployment.
Table. Comparison of volume aspirated by syringes and the Penumbra pump MAX.
For the experiment using a larger syringe to observe
the changes in hydrodynamic characteristics of water
aspiration, the plateau phases in the 60-mL VacLok
syringe and 60 mL initial volume of the 100-mL syringe
were equal, but the mean flow rates slightly differed
(p < 0.001), probably due to the different materials and
designs of both syringes.
The increase in syringe volume extended the duration
of the plateau phase without altering the duration of the
acceleration phase and deceleration phase and the flow
rate. Since the volume of fluid aspirated determined
phases, aspiration should be terminated before the
deceleration phase, which is 5 mL before the full capacity
(60, 70, 80, or 90 mL) of the 100-mL syringe in water
aspiration. The increase in syringe volume was equal
to the increase in the plateau phase volume. However,
a large, lockable syringe is currently not manufactured,
and the use is also limited to interventionists who have
enough strength to pull the syringe under a vacuum.
For every 10-mL increase in syringe volume, the plateau
phase time was extended by 2 s in water aspiration
(Table). Because of this linear correlation, we postulated
that for every 10-mL decrease in syringe volume,
the plateau phase time would be reduced by 2 s until
the plateau phase vanished in a ≤20-mL syringe. This
hypothesis is consistent with the low percentage (59%)
of recanalisation by a 20-mL syringe manual aspiration
thrombectomy.[7]
Interventionists can now consider the advantages and
disadvantages of the 60-mL VacLok syringe and the
28.5 inHg Penumbra Pump MAX regardless of the
comparable flow rates. Syringes are cost-effective,[4]
quick and straightforward to assemble, and easy to use[8];
however, they do require strength to create negative
pressure and have a short plateau phase, demanding
multiple disassembly and reassembly cycles in multiple
aspirations. The aspiration pump has a high capacity
with an extended constant flow rate without the need
for reassembly, but it requires preparation time for the
assembly of the apparatus and for the negative pressure
to reach 28.5 inHg before aspiration can be initiated.
Since this study was an in vitro experiment based on
water aspiration in a free-flow model, it reflects the real
treatment of mechanical thrombectomy in a limited way,
as blood has higher viscosity, which may result in lower
aspiration rates and a less precipitous acceleration phase.
The free-flow model of this study also could not reflect
full-clot engagement in the real thrombectomy, which
would increase the effective aspiration time. However,
partial clot engagement or clot dislodging could be
encountered in real-life treatment, creating a free flow
similar to this model. Despite the above limitations, the
aspiration rate created by both syringes and the pump
was shown to have the same characteristic acceleration
and plateau phases. Future research should consider
using alternative blood-like fluid, or in vivo experiments
should be conducted, focusing on finding the syringe
aspiration termination volume. Syringes should be
designed to indicate the termination volume and to have
high capacity while being labour-saving in the meantime.
In conclusion, interventionists can consider the
advantages and disadvantages of the two negative
pressure generators regardless of the comparable
aspiration power in the treatment of acute ischaemic
stroke. Moreover, the increase in syringe volume directly
increases the time of effective aspiration without altering
the aspiration force.
REFERENCES
1. Kang DH, Hwang YH, Kim YS, Park J, Kwon O, Jung C. Direct
thrombus retrieval using the reperfusion catheter of the penumbra
system: Forced-suction thrombectomy in acute ischemic stroke.
AJNR Am J Neuroradiol. 2011;32:283-7. Crossref
2. Turk AS, Spiotta A, Frei D, Mocco J, Baxter B, Fiorella D,
et al. Initial clinical experience with the adapt technique: A
direct aspiration first pass technique for stroke thrombectomy. J
Neurointerv Surg. 2014;6:231-7. Crossref
3. Humphries W, Hoit D, Doss VT, Elijovich L, Frei D, Loy D, et al.
Distal aspiration with retrievable stent assisted thrombectomy
for the treatment of acute ischemic stroke. J Neurointerv Surg.
2015;7:90-4. Crossref
4. Gross BA, Jadhav AP, Jovin TG, Jankowitz BT. Dump the
pump: Manual aspiration thrombectomy (MAT) with a syringe is
technically effective, expeditious, and cost-efficient. J Neurointerv
Surg. 2018;10:354-7. Crossref
5. Simon SD, Grey CP. Hydrodynamic comparison of the Penumbra
system and commonly available syringes in forced-suction
thrombectomy. J Neurointerv Surg. 2014;6:205-11. Crossref
6. McTaggart RA, Tung EL, Yaghi S, Cutting SM, Hemendinger M,
Gale HI, et al. Continuous aspiration prior to intracranial vascular
embolectomy (CAPTIVE): A technique which improves outcomes.
J Neurointerv Surg. 2017;9:1154-9. Crossref
7. Jankowitz B, Grandhi R, Horev A, Aghaebrahim A, Jadhav A,
Linares G, et al. Primary manual aspiration thrombectomy (MAT)
for acute ischemic stroke: safety, feasibility and outcomes in 112
consecutive patients. J Neurointerv Surg. 2015;7:27-31. Crossref
8. Kang DH, Park J. Endovascular stroke therapy focused on stent
retriever thrombectomy and direct clot aspiration: Historical review
and modern application. J Korean Neurosurg Soc. 2017;60:335-47. Crossref
| Attachment | Size |
|---|---|
| v24n1_Comparisonof.pdf | 500.38 KB |