
Decommissioned Computed Tomography Gantry Modified into Play Equipment to Promote Child-friendly Imaging
BRIEF COMMUNICATION
Decommissioned Computed Tomography Gantry Modified into Play Equipment to Promote Child-friendly Imaging
GE Punnen1, S Gibikote1, P Deodhar2, SN Keshava3
1 Department of Radiodiagnosis, Division of Clinical Radiology, Christian Medical College, Vellore, India
2 Office for the Promotion of Research & Writing, Principal’s Office, Carman Block, Christian Medical College, Vellore, India
3 Department of Interventional Radiology, Division of Clinical Radiology, Christian Medical College, Vellore,
India
Correspondence: Dr SN Keshava, Department of Interventional Radiology, Division of Clinical Radiology, Christian Medical College, Vellore, India. Email: shyamkumar.n.keshava@gmail.com
Submitted: 7 Apr 2021; Accepted: 3 Aug 2021.
Contributors: All authors designed the study, acquired the data, analysed the data, drafted the manuscript, and critically revised the manuscript
for important intellectual content. All authors had full access to the data, contributed to the study, approved the final version for publication, and
take responsibility for its accuracy and integrity.
Conflicts of Interest: All authors have disclosed no conflicts of interest.
Funding/Support: This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Ethics Approval: No patients were treated during course of this study. Individuals in the photographs (or their parent/guardian) provided written consent for their publication.
Acknowledgement: We would like to thank Dr Praveen Kumar C for the schematic diagrams and GRK Medifabs, Vellore, India, for contributing to the design and construction of the prototype.
BACKGROUND
A distinct set of challenges is involved in imaging
children.[1] Various imaging modalities require the patient
to lie motionless inside a gantry. While this period is
relatively short for a computed tomography (CT) study,
it can be as long as 15 to 60 minutes for a magnetic
resonance imaging (MRI) study. The experience of lying
within the unfamiliar, enclosed structure of a gantry,
while simultaneously exposed to loud and unpleasant
noises, can be extremely overwhelming for patients.
This is particularly challenging for young patients, and
can result in uncooperative or disruptive behaviour. This
behaviour results in lower imaging quality and increased
stress among technologists performing the study; thus,
the efficiency of imaging services is decreased.[1] [2]
Depending on the age of the child, various techniques,
including pharmacological and non-pharmacological interventions, can be employed to obtain high-quality
images and prevent repeat examinations. Approximately
60% to 100% of children aged 4 to 6 years who undergo
radiological examinations require some form of
pharmacological intervention, such as general anaesthesia
or sedation, in order to achieve motionless imaging.[3]
Although adverse effects of general anaesthesia are rare,
there are disadvantages (and costs), including the need
for a team of anaesthetists, additional time required, and
necessary space for care before and after the procedure.
Therefore, it is prudent to minimise the use of sedation or
general anaesthesia.[4] Non-pharmacological techniques
include mock scanners, an attractive child-friendly
environment, distraction techniques, preparatory videos,
colouring books, virtual reality apps, assistance from
child life specialists, or even trained animals.[5] These can
play a role in decreasing, or in some cases, mitigating
the need for sedation or general anaesthesia. However, in resource limited settings, there is little or no access to
many of these techniques. We herein describe a novel
method to introduce familiarity to CT or MRI gantries
by modifying a decommissioned CT gantry into a play
structure.
MODIFIED DECOMMISSIONED CT GANTRY
Design and Construction
The outer case of a CT machine referred to as a CT gantry, was selected for modification. The aim was to innovate it
in such a manner that it would appeal to young children
and be easily accessible to them. In consultation with
engineering experts, it was modified into a slide, a play
structure that most children are familiar with (Figures 1 and 2).
Figure 1. Schematic diagrams of a decommissioned computed tomography gantry modified as play equipment for children undergoing
imaging procedures. (a) Front, (b) front-oblique, and (c) side views were used to aid the technical team during construction.
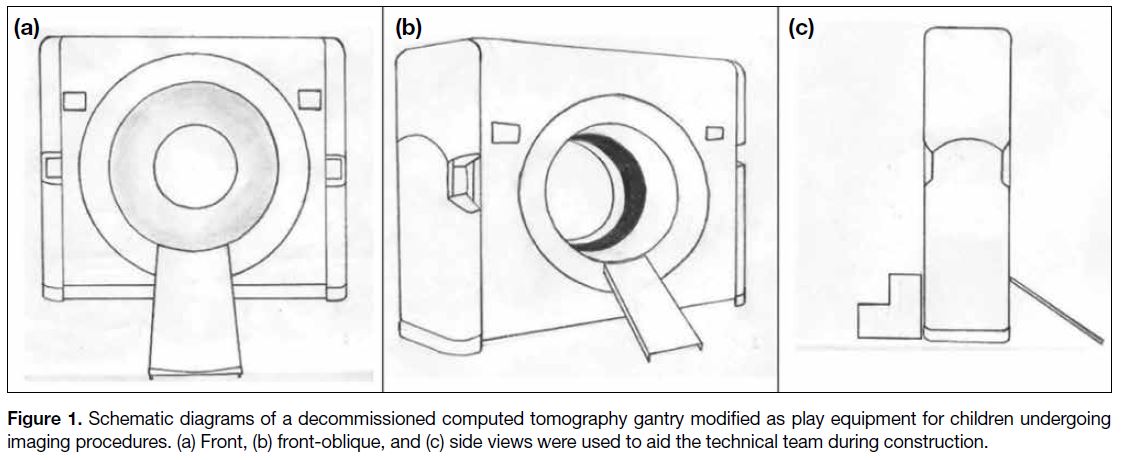
Figure 2. Photographs (a, b) showing children playing in the modified computed tomography gantry kept in the open patient waiting area.

As part of the modifications, the working parts of the gantry were removed from the inside. Metal scaffolding was added to the base of the gantry to provide stability to
the remaining light-weight structure. A short metal slide
was positioned at the front, leading from the opening in the
gantry, which became a ‘tunnel’ for the children. Small
steps were placed at the opposite end of the opening. The
height and size of the slide and steps were aligned to the
CT gantry and welded to the modified shell. Because the
slide and steps were quite low (approximately 60 cm),
no side railings were required. The original light grey
colour of the gantry was maintained, and the slide and
steps were painted more brightly (green) to visually
appeal to children. Some stickers were also added to
the gantry enhance the visual appeal. The cost of the
modifications was approximately US$150. The structure
requires only regular external cleaning and incurs no
other maintenance costs.
Safety
Safety was paramount. We ensured that there were no sharp objects or edges. Any small openings on the
surface, where switches or other parts had been removed,
were covered with plastic. The structure was stable and
sufficiently heavy, so it did not require any additional
fixing to the floor. Notices describing the apparatus
were attached to the gantry, with a specific message
addressing potential fears of parents that there were
no active or radiation-emitting components, as well as
instructions for use. As with all play structures, guardians
are expected to supervise their children. The modified
gantry was placed near the patient waiting area and was
not monitored by staff, although the area was in view of
a closed-circuit security camera. At the time of writing,
the decommissioned gantry has been in use for >2 years.
It is a very popular attraction that children queue to
use. There have been no untoward incidents during this
period, nor has the equipment required any repair.
Strengths and Limitations, and Comparison
with Alternatives
To the best of our knowledge, this is the first time
that a decommissioned CT gantry has been modified
to a play structure to familiarise children to gantries.
Barnea-Goraly et al[6] used a foldable toy tunnel, hat box,
foam padding and a vibrating massage mat to create an
inexpensive mock scanner for approximately US$80.
The authors observed that the success rates for high-quality
scans using a commercial mock scanner were not
significantly different from using their economical play
tunnel modification simulating the MRI environment,
thus they recommended this modification for use in
low resource settings. Compared with the toy tunnel of
Barnea-Goraly et al,[6] our modified CT gantry is more
realistic.
There are commercially available mock MRI gantry
models, which include a moving table and audio output
that simulates the noises and vibrations of an MRI
experience. This setup requires a separate room with an
electrical supply and operation by trained staff, which
may not be feasible in resource- and space-limited
settings.
A CT gantry was selected because it provides a life-size model of the imaging experience, but is smaller and
more convenient for our purposes than an MRI gantry.
Our centre retained the outer cover of a decommissioned
CT scanner, but the necessary parts could be obtained
from a third-party vendor. The parts required are
substantially cheaper than a commercially available
mock MRI gantry.
The modification of a decommissioned CT gantry into
a familiar play structure is our centre’s first attempt at
creating such a prototype to aid child-friendly imaging.
Further improvisation in the device could include battery-operated,
automated commands within the gantry.
CONCLUSION
We have shared our experience in developing and
converting a decommissioned CT gantry into a play
structure which provides familiarity to children before
undergoing imaging procedures. We believe this
adds to the non-pharmacological strategies for child-friendly
imaging, especially in situations where space
and resources are limited. Further research is required
to investigate whether this alternate calming method
reduces the need for anaesthesia for children undergoing
imaging procedures.
REFERENCES
1. Thukral BB. Problems and preferences in pediatric imaging. Indian J Radiol Imaging. 2015;25:359-64. Crossref
2. Barkovich MJ, Xu D, Desikan RS, Williams C, Barkovich AJ. Pediatric neuro MRI: tricks to minimize sedation. Pediatr Radiol. 2018;48:50-5. Crossref
3. Runge SB, Christensen NL, Jensen K, Jensen IE. Children centered care: minimizing the need for anesthesia with a multi-faceted concept for MRI in children aged 4-6. Eur J Radiol. 2018;107:183-7. Crossref
4. Arlachov Y, Ganatra RH. Sedation/anaesthesia in paediatric
radiology. Br J Radiol. 2012;85:e1018-31. Crossref
5. Raschle NM, Lee M, Buechler R, Christodoulou JA, Chang M, Vakil M, et al. Making MR imaging child’s play — pediatric neuroimaging protocol, guidelines and procedure. J Vis Exp. 2009;29:1309. Crossref
6. Barnea-Goraly N, Weinzimer SA, Ruedy KJ, Mauras N, Beck RW,
Marzelli MJ, et al. High success rates of sedation-free brain MRI
scanning in young children using simple subject preparation
protocols with and without a commercial mock scanner — the
Diabetes Research in Children Network (DirecNet) experience.
Pediatr Radiol. 2014;44:181-6. Crossref