
Perilesional Sclerosis Associated with Dreaded Black Lines in Incomplete Atypical Femoral Fractures after Antiresorptive Therapy
ORIGINAL ARTICLE
Hong Kong J Radiol 2026;29:Epub 27 February 2026
Perilesional Sclerosis Associated with Dreaded Black Lines in
Incomplete Atypical Femoral Fractures after Antiresorptive Therapy
KC Wong1, GJW Cheok1, SB Koh1, P Chandra Mohan2, MA Png2, TS Howe1 YH Ng1
1 Department of Orthopaedic Surgery, Singapore General Hospital, Singapore
2 Department of Diagnostic Radiology, Singapore General Hospital, Singapore
Correspondence: Dr KC Wong, Department of Orthopaedic Surgery, Singapore General Hospital, Singapore. Email: khaicheong.wong@mohh.com.sg
Submitted: 12 June 2024; Accepted: 8 September 2025. This version may differ from the final version when published in an issue.
Contributors: SBK and TSH designed the study. KCW and GJWC acquired and analysed the data. All authors drafted the manuscript and
critically revised the manuscript for important intellectual content. All authors had full access to the data, contributed to the study, approved the
final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of Interest: All authors have disclosed no conflicts of interest.
Funding/Support: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data Availability: All data generated or analysed during the present study are available from the corresponding author on reasonable request.
Ethics Approval: This research was approved by the SingHealth Centralised Institutional Review Board (Ref No.: 2019/2668). The requirement
for informed patient consent was waived by the Board as non-identifiable data were used and due to the retrospective nature of the research.
Abstract
Introduction
This study aimed to describe the demographic, clinical, and radiological features of sclerosis adjacent
to ‘dreaded black lines’ or radiolucent fracture lines (RFLs) in atypical femoral fractures (AFFs) associated with
antiresorptive therapy.
Methods
We reviewed radiographs acquired in our institution in Singapore between 2004 and 2020 from 100 femurs
with AFFs, assessing the appearance and location of lesions, and the presence of endosteal or periosteal thickening.
Demographic data, type and duration of antiresorptive therapy, and progression to complete fracture or need for
prophylactic stabilisation were analysed. The cohort was subdivided into three groups: Group 1A included AFFs
with an RFL and perilesional sclerosis; Group 1B included AFFs with an RFL but without perilesional sclerosis;
and Group 2 included AFFs without an RFL.
Results
A total of 17 sclerotic RFLs were identified. The majority were non-linear in appearance. Most were located
in the subtrochanteric (41.2%) and proximal diaphyseal regions (35.3%), and all were associated with endosteal
or periosteal thickening. All sclerotic RFLs occurred in patients with a mean age of 69 years. Sixteen cases (94.1%)
had a history of bisphosphonate use, while one case had received denosumab. The mean duration of antiresorptive
therapy was 66 months. Three cases (17.6%) progressed to complete fractures and six (35.3%) required prophylactic
fixation. No significant differences were observed among the three groups in terms of demographics, antiresorptive
therapy, or surgical intervention.
Conclusion
We describe perilesional sclerosis as a previously unrecognised radiological feature adjacent to RFLs
in AFFs, with distinctive characteristics. It occurs in approximately one-third of RFLs. Further research is needed
to elucidate its pathophysiological and prognostic implications.
Key Words: Biphosphonates; Femoral fractures; Sclerosis
中文摘要
抗骨質吸收治療後不完全性非典型股骨骨折伴隨怪樣黑線周圍硬化
黃啟翔、石佳偉、許鑽美、P Chandra Mohan、方明愛、侯德生、黃勇輝
引言
本研究旨在描述接受抗骨質吸收治療的非典型股骨骨折(atypical femoral fractures, AFF)中,鄰近「怪樣黑線」或透光骨折線(radiolucent fracture lines, RFL)的骨質硬化之人口統計學、臨床及放射學特徵。
方法
我們回顧性分析了2004年至2020年間在新加坡我院就診的100例AFF患者之X光片,評估病變的形態與位置,以及是否存在骨內膜或骨外膜增厚。同時分析患者的人口統計學資料、抗骨質吸收治療的類型與持續時間,以及是否進展為完全性骨折或需要預防性固定。根據影像表現將患者分為三組:1A組為伴有RFL及病灶周圍硬化的AFF;1B組為伴有RFL但無病灶周圍硬化的AFF;2組為無RFL的AFF。
結果
共發現17例硬化性RFL,多呈非線性形態。大多位於股骨大轉子下區(41.2%)及近端骨幹區(35.3%),所有病例均伴隨骨內膜或骨外膜增厚。硬化性RFL患者的平均年齡為69歲,其中16例(94.1%)有雙磷酸鹽使用史,1例曾接受地舒單抗治療。抗骨質吸收治療的平均持續時間為66個月。3例(17.6%)進展為完全性骨折,6例(35.3%)需接受預防性內固定。三組患者在人口統計學特徵、抗骨質吸收治療或手術介入方面均無顯著差異。
結論
我們描述了病灶周圍硬化,此為一種先前未被識別的AFF中RFL附近之放射學特徵,具有獨特的表現形式。其發生率約佔RFL病例的三分之一。需進一步研究以闡明其病理生理機制及預後意義。
INTRODUCTION
Atypical femoral fractures (AFFs) were first recognised
as a distinct clinical entity following multiple clinical
reports, yet their pathophysiology and clinical
characteristics remain incompletely understood.[1] [2]
Over time, our understanding of AFFs has evolved,
as reflected in ongoing efforts by a task force of the
American Society for Bone and Mineral Research
(ASBMR) to refine diagnostic criteria.[1] [2] Major features
used to define AFFs were first established in 2010 and
included fractures following low-energy or no trauma,
transverse fractures originating from the lateral cortex
which may become oblique medially, complete fractures
with a medial spike, and incomplete fractures involving
only the lateral cortex, with minimal or no comminution
and localised periosteal or endosteal thickening of the
lateral cortex.[1] Minor features associated but not required
for diagnosis include generalised femoral diaphyseal
cortical thickening, unilateral or bilateral prodromal pain
in the groin or thigh, incomplete or complete fractures of
both femoral diaphyses, and delayed fracture healing.[1]
In 2014, new epidemiological studies and clinical data
prompted the ASBMR to revise the definition of AFFs, emphasising their diaphyseal location and requiring at
least four of the five major features for diagnosis.[2] This
refined definition provides a more precise framework for
identifying AFFs and distinguishing them from typical
osteoporotic femoral fractures.2 This reflects the dynamic
and evolving nature of our understanding of AFFs and
highlights that much remains unknown, including the
identification of potential novel clinical and radiological
features and their implications for patient management.
Radiological studies have also expanded our
understanding of AFFs, particularly when Mohan et al[3]
described multifocal endosteal thickening along the
femoral diaphysis in bisphosphonate-related AFFs,
highlighting its association with a periosteal beak and/or
a ‘dreaded black line’, also referred to as a radiolucent
fracture line (RFL). These features were associated
with an increased risk of progression to fracture.[3] A
subsequent study by Png et al[4] demonstrated that when
an RFL is present, the lesion is likely to persist, either
remaining static or progressing to a displaced fracture.
The significance of RFLs was also emphasised in the
2015 position statement by the Korean Society for Bone and Mineral Research, which recommended prophylactic
femoral nailing in the presence of an RFL, especially
when located in the subtrochanteric region.[5]
Despite these insights, gaps remain in the literature, as
not all RFLs progress to complete fractures and there are
no clear discerning features to guide when prophylactic
fixation is indicated. During our review of patients
with AFFs, we observed a previously undescribed
radiological feature: perilesional sclerosis—an area
of sclerosis closely associated with the presence of an
RFL seen in an incomplete AFF. This finding, distinct
from previously reported radiological features of AFFs,
may have implications for understanding bone stability,
fracture progression, and management strategies, as
sclerosis has previously been suggested to be associated
with fatigue fractures and delayed fracture healing.[6]
Although with established diagnostic criteria and the
recognition of RFLs as high-risk markers, it remains
unclear why not all RFLs progress to complete fractures
or ultimately require intervention. To date, no study has
described the presence or significance of perilesional
sclerosis in relation to RFLs in AFFs. Our study aimed
to address this gap by identifying and characterising
this radiological feature in association with RFLs in
incomplete AFFs, and by exploring its potential clinical
implications.
METHODS
Study Cohort
We retrospectively reviewed plain radiographs of
cases of incomplete AFFs in patients presenting to our
institution in Singapore while receiving bisphosphonate
therapy between 2004 and 2020. These cases were
retrieved from our institutional AFF registry, which
includes patients exhibiting features of AFF that have
not yet progressed to a complete fracture.
We reviewed all available plain radiographs of the
AFFs, as well as those of the contralateral femur when
available. Perilesional sclerosis was defined as a linear
area of sclerosis observed on either side of an RFL. All
anteroposterior and lateral views were obtained using
standard radiographic techniques, and all analysed
fractures met the ASBMR criteria for an AFF.[3] [4]
The study cohort of 100 AFFs was subsequently divided
into three groups: Group 1A included AFFs with an RFL
and perilesional sclerosis; Group 1B included AFFs with
an RFL but without perilesional sclerosis; and Group 2 included AFFs without an RFL.
We also analysed age data and collected information on
the type and duration of bisphosphonate therapy. Patients
were followed up for sequelae, including progression to
complete fracture or subsequent prophylactic fixation.
Prophylactic fixation was performed in cases of
persistent pain at the site of AFFs, while surgical fixation
was performed for patients who progressed to complete
fractures.
Image Analysis
All radiographs were reviewed for the presence of RFLs
with adjacent sclerosis using Vue Motion (Carestream
Health, Rochester [NY], US), and independently assessed
by two authors (SBK and TSH), each with over 20 years of
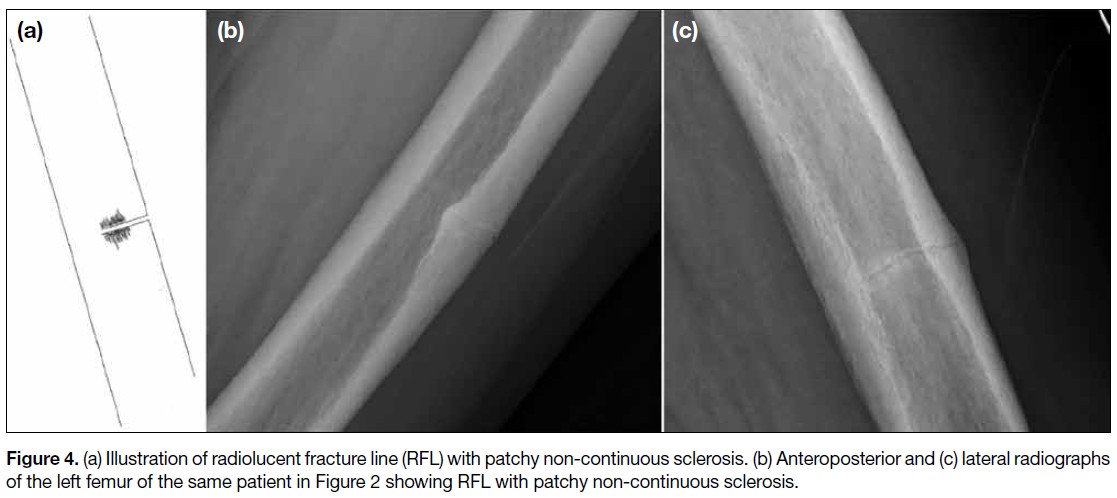
clinical orthopaedic experience. RFLs were categorised
into one of four patterns: (1) RFL without sclerosis
(Figure 1); (2) RFL with linear sclerosis (Figure 2);
(3) RFL with patchy continuous sclerosis (Figure 3); and
(4) RFL with patchy non-continuous sclerosis (Figure 4).
Figure 1. (a) Illustration of radiolucent fracture line (RFL) without sclerosis. (b) Anteroposterior and (c) lateral radiographs of the left femur
showing an RFL without sclerosis.
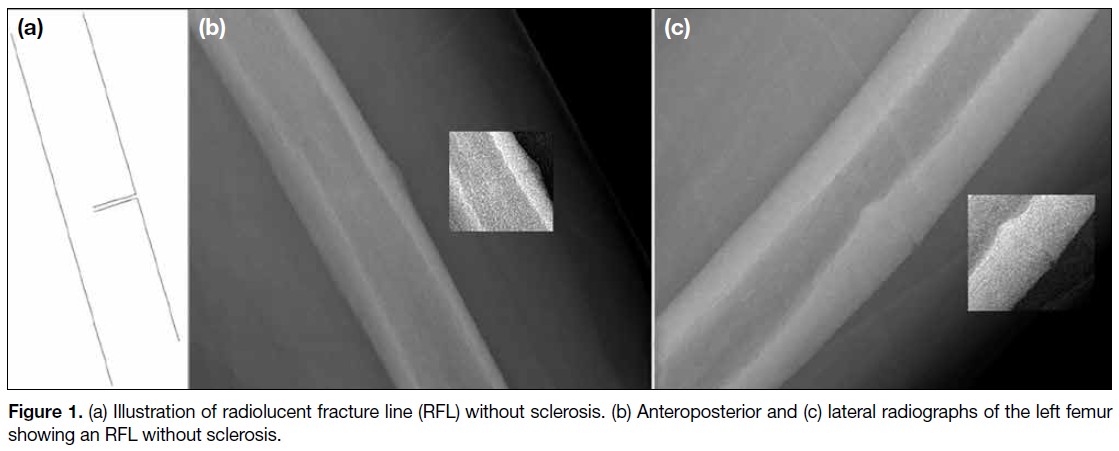
Figure 2. (a) Illustration of radiolucent fracture line
(RFL) showing linear sclerosis. (b) Lateral radiograph
of the left femur showing an RFL with linear sclerosis.
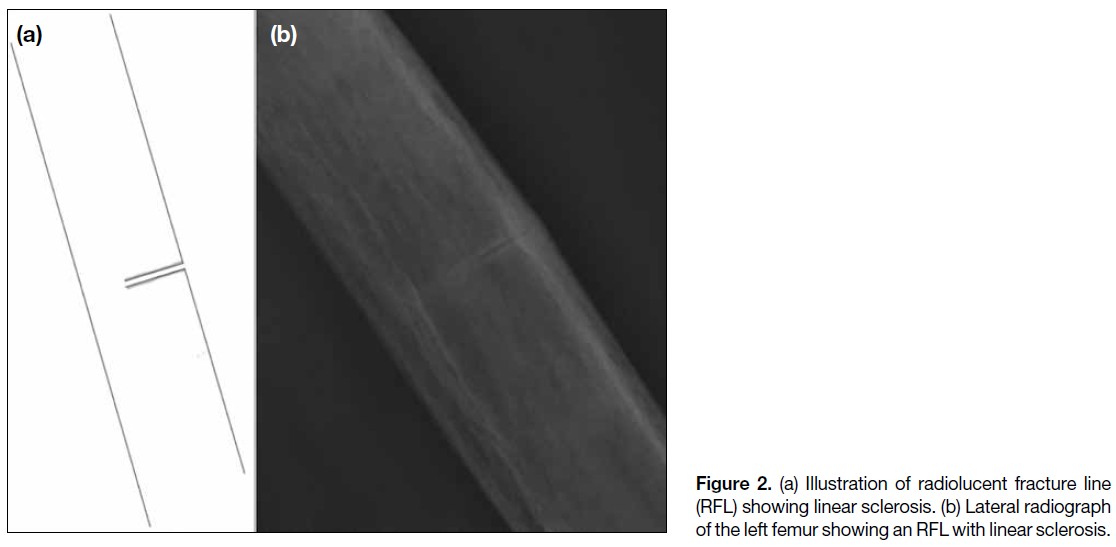
Figure 3. (a) Illustration of radiolucent fracture line (RFL) with patchy continuous sclerosis. (b) Anteroposterior and (c) lateral radiographs of
the left femur showing an RFL with patchy continuous sclerosis.
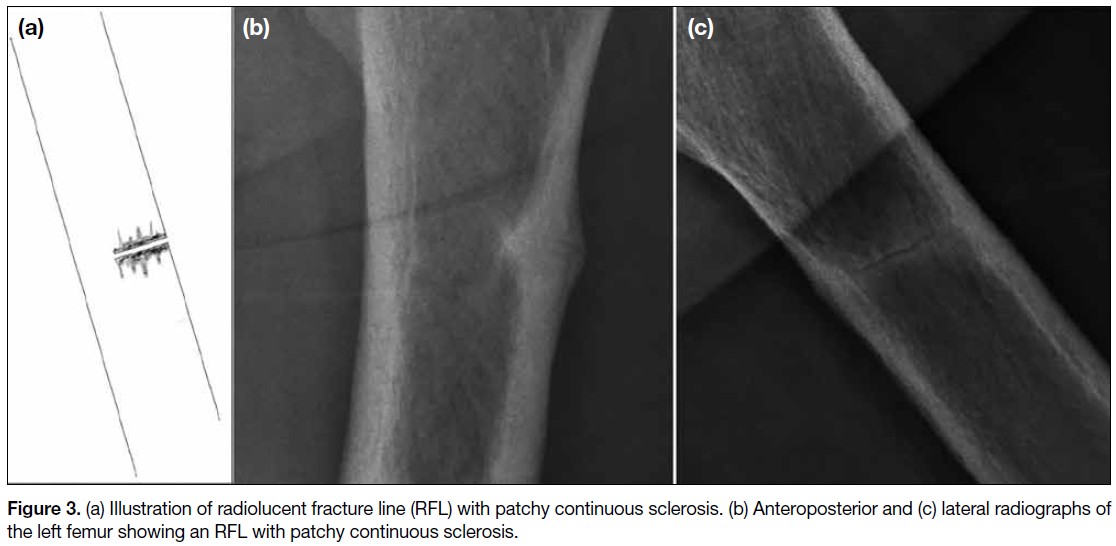
Figure 4. (a) Illustration of radiolucent fracture line (RFL) with patchy non-continuous sclerosis. (b) Anteroposterior and (c) lateral radiographs
of the left femur of the same patient in Figure 2 showing RFL with patchy non-continuous sclerosis.
We recorded the location of each lesion, along with
the presence or absence of focal endosteal or periosteal
thickening. Cases were followed up until fixation was
required or a complete fracture occurred. Lesions were
classified as being located in either the subtrochanteric or
diaphyseal region, and further subdivided into proximal,
middle, or distal thirds. Observations were collected
independently by each of the same two authors and
correlated. In the event of any discrepancies, a senior
radiologist was consulted to provide a final decision.
Statistical Analysis
Pearson’s Chi squared test was used to compare
categorical data, while one-way analysis of variance was
employed to analyse continuous variables. Statistical
analyses were performed using SPSS (Windows
version 23.0; IBM Corp, Armonk [NY], US). Statistical
significance was defined as p < 0.05.
RESULTS
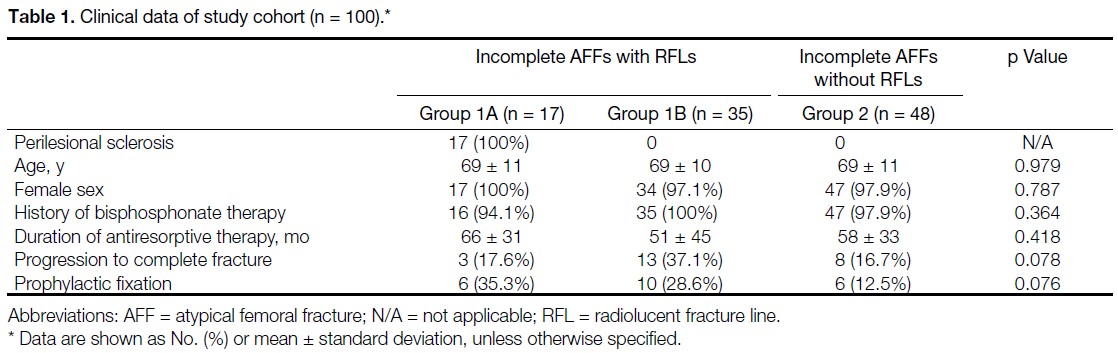
There were 100 radiographs of AFFs from 80 cases
available for review. Demographic and clinical data of
the study cohort are summarised in Table 1. There were
17 femurs in Group 1A, 35 femurs in Group 1B, and
48 femurs in Group 2. All 17 femurs with perilesional
sclerosis were independently identified by the two
authors previously described. There were no significant
differences among the three groups in terms of patient
demographics (age: p = 0.979); the patients were predominantly female and Asian. All had a history of
bisphosphonate use, except for two AFF cases with a
history of denosumab use only (one in Group 1A and
one in Group 2). There were no significant differences
in the duration of antiresorptive therapy (p = 0.418),
progression to complete fracture (p = 0.078), or
subsequent prophylactic fixation (p = 0.076) among the
three groups. The radiographic finding of perilesional
sclerosis was observed in 17 of the 100 femurs (17%),
with bilateral involvement in three patients who were all
female with a mean age of 66 years; two were Chinese
(88.2%) and the remaining patient was of Indian descent. The mean (± standard deviation) duration of
bisphosphonate use was 66 ± 31 months (range, 4-120).
Only one femur in Group 1A was from a patient with a
history of denosumab use without prior bisphosphonate
therapy. Bisphosphonate treatment was discontinued
upon diagnosis of AFF in all patients. Three femurs
(17.6%) subsequently progressed to complete fractures,
while six incomplete fractures required prophylactic
fixation (35.3%). The mean (± standard deviation) time
to surgical fixation or prophylactic fixation from the date
of presentation with perilesional sclerosis was 9 ± 12
months.
Table 1. Clinical data of study cohort (n = 100).
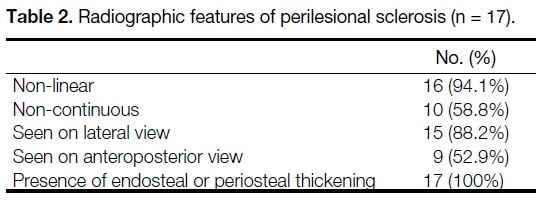
The radiographic features of perilesional sclerosis in
Group 1A are summarised in Table 2. Each sclerotic
lesion was observed in an incomplete AFF and only
in the presence of an RFL. Perilesional sclerosis was
identified on lateral views in 15 femurs (88.2%), while
only nine femurs (52.9%) demonstrated sclerosis on
anteroposterior views. The lesions were mainly located
in the subtrochanteric region (n = 7, 41.2%), followed by
the proximal diaphyseal region (n = 6, 35.3%) and the
mid-diaphyseal region (n = 4, 23.5%). All lesions were
associated with either adjacent endosteal thickening or
periosteal thickening. Of the 17 lesions with perilesional
sclerosis, 16 (94.1%) were RFLs with patchy sclerosis
of varying widths along either side of the fracture line,
and 10 (58.8%) demonstrated patchy non-continuous
sclerosis.
Table 2. Radiographic features of perilesional sclerosis (n = 17).
Among the 17 femurs with sclerotic RFLs, three had
earlier radiographs (mean, 56.4 months, range, 0.5-96.3)
showing an RFL without adjacent sclerosis, indicating
that perilesional sclerosis developed later. Once sclerosis
appeared, it persisted in all subsequent follow-up
radiographs. For the eight femurs that did not undergo
surgery, the mean duration between the first presentation
of RFL with perilesional sclerosis and the last available
radiograph was 31 ± 22 months (range, 0-57.6). Follow-up
was achieved for 100% of the 17 lesions, with a mean
follow-up duration of 72 ± 45 months (range, 8-184).
Regarding inter-observer variability, there was complete
agreement between both readers on the presence and
pattern of sclerosis.
DISCUSSION
Our study describes the presence of perilesional sclerosis
adjacent to the RFL, previously described by Png et al,[4]
and the radiological progression of AFFs in which
the RFL is recognised as the penultimate radiological
feature before progression to a complete fracture. We
observed that an RFL can be associated with, or may later
develop, perilesional sclerosis. This radiological feature
has not previously been documented in AFFs, which
are predominantly located between the subtrochanteric region and mid-diaphyseal regions of the femur, may be
bilateral and are consistently associated with endosteal or
periosteal thickening. In our study, perilesional sclerosis
appears to occur in approximately one-third of AFFs
with an RFL, and is usually seen on lateral radiographic
views, and occasionally on anteroposterior radiographic
views. While the variability in its appearance and its
significance remain largely unstudied, and descriptions in
the literature are scarce, our study presents observations
that may enhance our understanding of this entity.
AFFs are considered to be ‘tensional’ stress fractures,
typically initiating along the upper two-thirds of the
lateral femoral shaft corresponding to regions subjected
to greater tensional forces.[7] Accordingly, RFLs are better
observed as linear structures across the femoral diaphysis
on lateral views. As perilesional sclerosis appears to
occur in association with RFLs, this may account for its
notably high prevalence on lateral views of the femoral
shaft.
In the majority of our cases, perilesional sclerosis was
observed only on the lateral views. In two cases with
both anterior and lateral cortical thickening, sclerosis
was visible on both anteroposterior and lateral views.
These findings suggest that, in most cases, perilesional
sclerosis may be related to viewing cortical thickening
at right angles to its long axis. However, in two cases,
perilesional sclerosis was seen on the anteroposterior
views despite cortical thickening being confined to the
lateral cortex. This suggests that, in these cases, there
was focal sclerosis at the intracortical fracture margins.
Radiologically, sclerosis at fracture sites has been
described as a feature of fracture non-union.[8] Although
sclerosis has been postulated to be associated with
avascular necrosis or reduced metabolic bone activity,[9]
it has also been linked to prolonged time to union.[10]
Perilesional sclerosis has been mentioned in some
cases of insufficiency fractures but is rarely described
in AFFs. Only a single study by McKenna et al[11]
described sclerosis in relation to AFFs, but only on
computed tomography scans without specific reference
to its relationship with RFLs. The fact that this feature
is observed only in a subset of incomplete AFFs with
variable continuity along the RFL, suggests that it may
represent a phase in the pathophysiological progression
of AFFs.
Perilesional sclerosis associated with cortical thickening
may resemble that seen in stress or fatigue fractures. However, cases with intracortical perilesional sclerosis
may represent an early phase of the process leading to
non-union. Fracture non-union is usually associated with
sclerosis at the fracture margins, and the two cases in our
cohort where sclerosis was confined to the lateral cortex
may represent non-union of the incomplete fracture, akin
to hypertrophic non-union involving the lateral cortex.
This may be the result of persistent tensile stresses that
inhibit bony union.[12] These lesions also appeared to
progress from an isolated RFL to an RFL with adjacent
sclerosis, with this radiographic feature persisting for a
mean duration of 31 ± 22 months. Perilesional sclerosis
may take considerable time to develop but can persist
long after initial presentation. We postulate that it could
represent the development of a chronic non-union state in
incomplete AFFs. Bisphosphonates such as alendronate
are known to have prolonged effects on osteoclast
function, and these may continue long after cessation of
therapy.[13]
Although there were no significant differences in the
proportion of cases that progressed to complete fracture
or required prophylactic fixation between Group 1A and
Group 1B, a higher rate of surgical fixation in Group 1B
was noted (65.7% vs. 52.9%). A histological study by
Schilcher et al[14] demonstrated signs of attempted healing
at the site of AFFs; however, the current literature does not
explain the pathological differences between AFFs that
eventually heal and those that do not. Future histological
studies could examine samples of perilesional sclerosis
to explore the underlying pathology and provide insights
into its clinical significance.
Strengths and Limitations
A strength of this study is the 100% follow-up rate
over a mid-term duration for a previously undescribed
radiological finding in AFFs. The main limitation is the
limited sample size of patients with perilesional sclerosis,
although this may reflect the low prevalence of AFFs
among patients on antiresorptive therapy. Additionally,
the predominance of female patients in the cohort
limited our ability to assess potential gender-related
differences. Another limitation is the irregular follow-up
of patients due to variation in individual physicians’
clinical practices and the retrospective nature of the
study. Longer-term, regularly scheduled follow-up with
standardised radiographic imaging should be considered
in future studies to better evaluate the relationship
between these lesions and fracture outcomes.
CONCLUSION
We describe perilesional sclerosis as a previously
unrecognised radiological feature along the RFL, in
incomplete AFFs with distinctive characteristics. Its
presence may suggest a state of non-union and was
observed in approximately one-third of cases with an
RFL. Further research involving larger cohorts could
shed light on its pathophysiological and prognostic
significance.
REFERENCES
1. Shane E, Burr D, Ebeling PR, Abrahamsen B, Adler RA,
Brown TD, et al. Atypical subtrochanteric and diaphyseal femoral
fractures: report of a task force of the American Society for Bone
and Mineral Research. J Bone Miner Res. 2010;25:2267-94.
Crossref
2. Shane E, Burr D, Abrahamsen B, Adler RA, Brown TD,
Cheung AM, et al. Atypical subtrochanteric and diaphyseal
femoral fractures: second report of a task force of the American
Society for Bone and Mineral Research. J Bone Miner Res.
2014;29:1-23.
Crossref
3. Mohan PC, Howe TS, Koh JS, Png MA. Radiographic features of
multifocal endosteal thickening of the femur in patients on long-term bisphosphonate therapy. Eur Radiol. 2013;23:222-7.
Crossref
4. Png MA, Mohan PC, Koh JS, Howe CY, Howe TS. Natural
history of incomplete atypical femoral fractures in patients after a prolonged and variable course of bisphosphonate therapy—a long-term radiological follow-up. Osteoporos Int. 2019;30:2417-28.
Crossref
5. Yang KH, Min BW, Ha YC. Atypical femoral fracture: 2015
position statement of the Korean Society for Bone and Mineral
Research. J Bone Metab. 2015;22:87-91.
Crossref
6. Hedge G, Thaker S, Botchu R, Fawcett R, Gupta H. Atraumatic
fractures of the femur. Br J Radiol. 2021;94:20201457.
Crossref
7. Koh JS, Goh SK, Png MA, Ng AC, Howe TS. Distribution
of atypical fractures and cortical stress lesions in the femur:
implications on pathophysiology. Singapore Med J. 2011;52:77-80.
8. Gharu E, John B. Nonunion of fractures: a review of epidemiology, diagnosis, and clinical features in recent literature. Indian J Orthop. 2024;58:1680-5.
Crossref
9. Jones W, Roberts RE. Pathological calcification and ossification in relation to Leriche and Policard’s theory. Proc R Soc Med. 1933;26:853-9.
Crossref
10. Schmidle G, Ebner HL, Klauser AS, Fritz J, Arora R, Gabl M.
Correlation of CT imaging and histology to guide bone graft
selection in scaphoid non-union surgery. Arch Orthop Trauma
Surg. 2018;138:1395-405.
Crossref
11. McKenna MJ, Heffernan E, Hurson C, McKiernan FE. Clinician
approach to diagnosis of stress fractures including bisphosphonateassociated
fractures. QJM. 2014;107:99-105.
Crossref
12. Andrzejowski P, Giannoudis PV. The ‘diamond concept’ for long
bone non-union management. J Orthop Traumatol. 2019;20:21.
Crossref
13. Stock JL, Bell NH, Chesnut CH 3rd, Ensrud KE, Genant HK,
Harris ST, et al. Increments in bone mineral density of the lumbar
spine and hip and suppression of bone turnover are maintained after
discontinuation of alendronate in postmenopausal women. Am J
Med. 1997;103:291-7.
Crossref
14. Schilcher J, Sandberg O, Isaksson H, Aspenberg P. Histology of 8 atypical femoral fractures: remodeling but no healing. Acta Orthop. 2014;85:280-6.
Crossref