
Perineural and Muscular Involvement in Recurrent Diffuse Large B-Cell Lymphoma Detected by Fluorine-18 Fluorodeoxyglucose Positron Emission Tomography/Computed Tomography: A Case Report
CASE REPORT
Hong Kong J Radiol 2026;29:Epub 26 February 2026
Perineural and Muscular Involvement in Recurrent Diffuse Large
B-Cell Lymphoma Detected by Fluorine-18 Fluorodeoxyglucose
Positron Emission Tomography/Computed Tomography: A Case
Report
JHY Lau, KK Ng, BT Kung
Nuclear Medicine Unit, Department of Diagnostic and Interventional Radiology, Queen Elizabeth Hospital,
Hong Kong SAR, China
Correspondence: Dr JHY Lau, Nuclear Medicine Unit, Department of Diagnostic and Interventional Radiology, Queen Elizabeth
Hospital, Hong Kong SAR, China. Email: hugh.lau@ha.org.hk
Submitted: 16 December 2024; Accepted: 5 September 2025. This version may differ from the final version when published in an issue.
Contributors: All authors designed the study. JHYL acquired the data. All authors analysed the data. JHYL drafted the manuscript. KKN and
BTK critically revised the manuscript for important intellectual content. All authors had full access to the data, contributed to the study, approved
the final version for publication, and take responsibility for its accuracy and integrity.
Conflicts of Interest: All authors have disclosed no conflicts of interest.
Funding/Support: This study received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Data Availability: All data generated or analysed during the present study are available from the corresponding author on reasonable request.
Ethics Approval: This study was approved by the Central Institutional Review Board of Hospital Authority, Hong Kong (Ref No.: CIRB-2024-313-4). The requirement for patient consent was waived by the Board as the patient was deceased and no contact information for next of kin
was available. The study involved retrospective review of anonymised clinical data only and posed no risk to subjects. All data were handled in
accordance with Hospital Authority policies on data privacy and security.
CASE PRESENTATION
A 79-year-old female with a past medical history of
hypertension and impaired fasting glucose presented to
our institution in April 2020 with a neck mass and fever.
She was an ex-smoker with no known drug allergies.
Following an ear, nose, and throat consultation, she was
diagnosed with stage 4B diffuse large B-cell lymphoma
(DLBCL). A biopsy of the left tonsil revealed high-grade
B-cell lymphoma, consistent with DLBCL. Further
evaluation including bilateral bone marrow aspiration
and bilateral trephine biopsy showed no evidence of
lymphoma involvement.
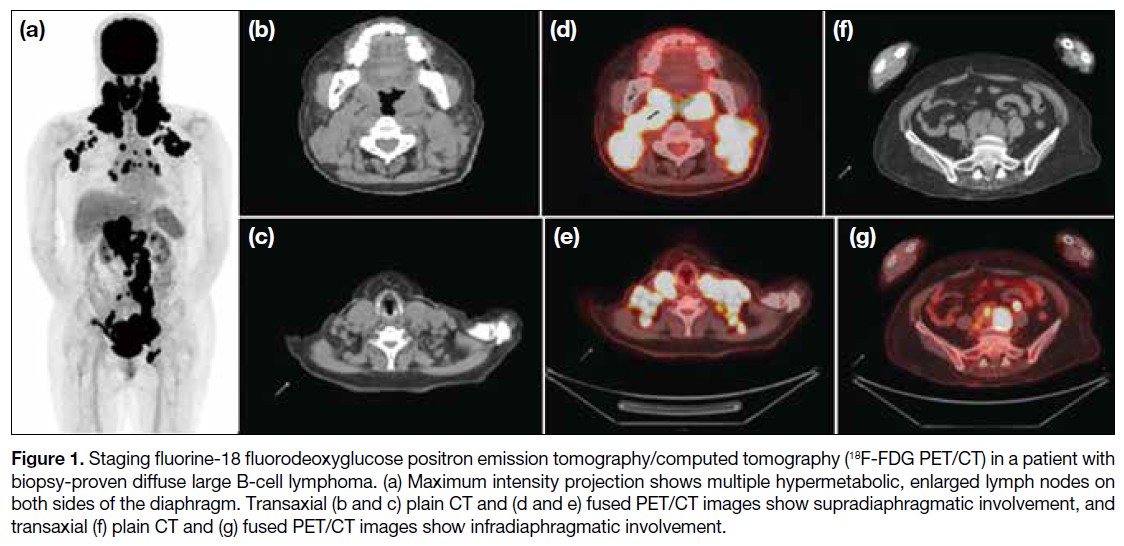
Staging fluorine-18 fluorodeoxyglucose positron
emission tomography/computed tomography (18F-FDG
PET/CT) revealed hypermetabolic lymphadenopathy on
both sides of the diaphragm, consistent with the biopsy-proven lymphoma, as well as hypermetabolic lesions in bilateral tonsils, confirming lymphomatous involvement
(Figure 1).
Figure 1. Staging fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) in a patient with
biopsy-proven diffuse large B-cell lymphoma. (a) Maximum intensity projection shows multiple hypermetabolic, enlarged lymph nodes on
both sides of the diaphragm. Transaxial (b and c) plain CT and (d and e) fused PET/CT images show supradiaphragmatic involvement, and
transaxial (f) plain CT and (g) fused PET/CT images show infradiaphragmatic involvement.
The patient commenced R-CHOP chemotherapy
(rituximab, cyclophosphamide, doxorubicin, vincristine,
and prednisone), receiving six cycles over 5 months.
The first cycle was administered at 50% dosage, with
subsequent cycles adjusted for tolerance and side-effects.
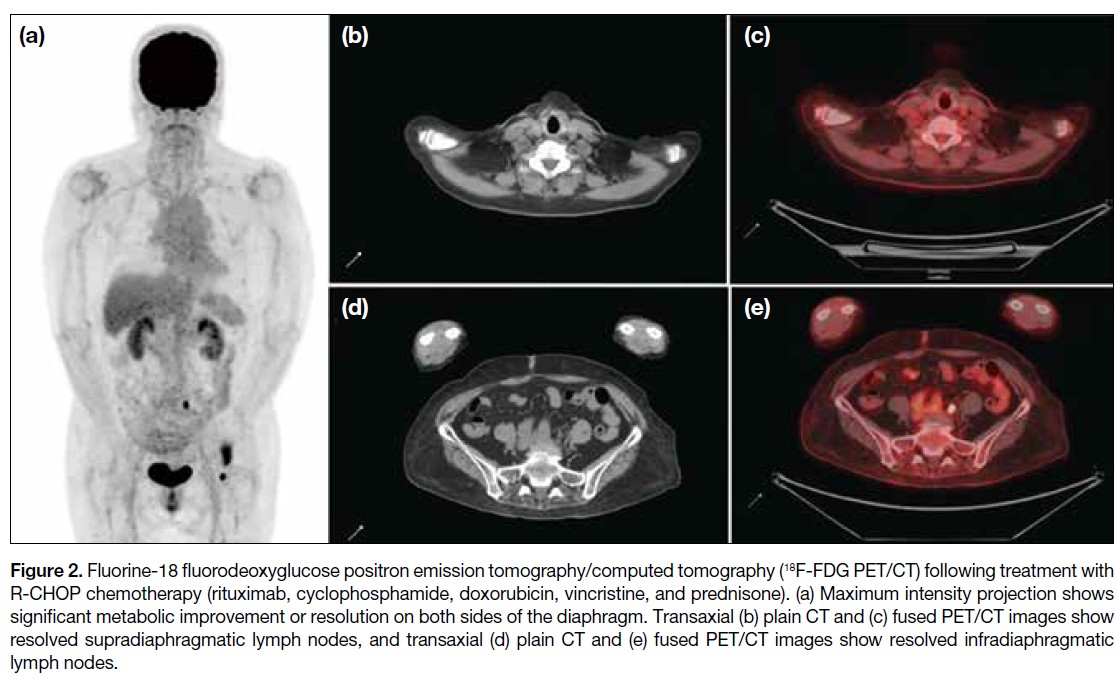
Following completion of the last cycle, an
end-of-treatment 18F-FDG PET/CT scan demonstrated
complete metabolic remission, with a Deauville score of
2 (Figure 2).
Figure 2. Fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) following treatment with
R-CHOP chemotherapy (rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone). (a) Maximum intensity projection shows
significant metabolic improvement or resolution on both sides of the diaphragm. Transaxial (b) plain CT and (c) fused PET/CT images show
resolved supradiaphragmatic lymph nodes, and transaxial (d) plain CT and (e) fused PET/CT images show resolved infradiaphragmatic
lymph nodes.
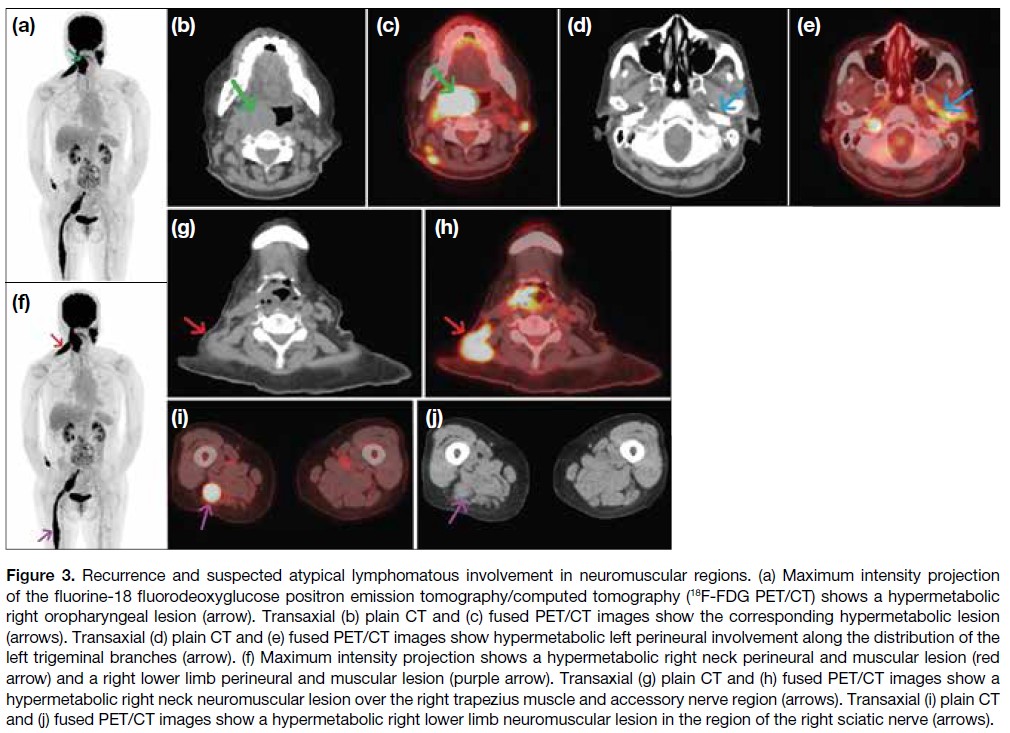
Five months after completing R-CHOP chemotherapy,
the patient developed a right neck mass and numbness
over the right side of her neck and right lower limb, with
muscle power graded at 2 out of 5. A CT scan revealed a
large soft tissue mass on the right side of the oropharynx, and biopsy confirmed DLBCL with CD20 positivity. A
subsequent 18F-FDG PET/CT scan for restaging revealed
a new hypermetabolic soft tissue mass in the right side
of the oropharynx, consistent with lymphomatous
involvement, with a Deauville score of 5. Notably, the scan also revealed new, multiple hypermetabolic
foci involving perineural and muscular involvements
in the bilateral head and neck regions and the right
proximal lower limb, raising suspicion for perineural
lymphomatous infiltration (Figure 3).
Figure 3. Recurrence and suspected atypical lymphomatous involvement in neuromuscular regions. (a) Maximum intensity projection
of the fluorine-18 fluorodeoxyglucose positron emission tomography/computed tomography (18F-FDG PET/CT) shows a hypermetabolic
right oropharyngeal lesion (arrow). Transaxial (b) plain CT and (c) fused PET/CT images show the corresponding hypermetabolic lesion
(arrows). Transaxial (d) plain CT and (e) fused PET/CT images show hypermetabolic left perineural involvement along the distribution of the
left trigeminal branches (arrow). (f) Maximum intensity projection shows a hypermetabolic right neck perineural and muscular lesion (red
arrow) and a right lower limb perineural and muscular lesion (purple arrow). Transaxial (g) plain CT and (h) fused PET/CT images show a
hypermetabolic right neck neuromuscular lesion over the right trapezius muscle and accessory nerve region (arrows). Transaxial (i) plain CT
and (j) fused PET/CT images show a hypermetabolic right lower limb neuromuscular lesion in the region of the right sciatic nerve (arrows).
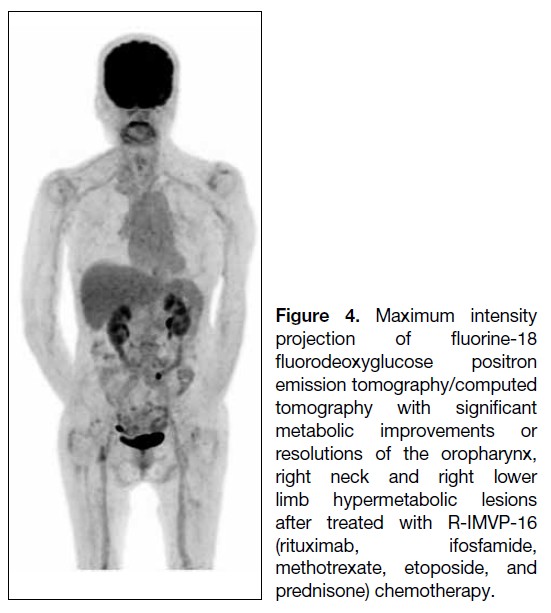
The patient subsequently received six cycles of
R-IMVP-16 (rituximab, ifosfamide, methotrexate,
etoposide, and prednisone) over 5 months. End-of-treatment 18F-FDG PET/CT showed metabolic
resolution of the right tonsillar/oropharyngeal mass and
other infiltrative perineural lesions in the neck region
and right lower limb, indicating a favourable treatment
response (Figure 4). Clinically, her numbness subsided,
with improved sensation in the previously affected
regions and right lower limb power improved to 4 out
of 5, consistent with the 18F-FDG PET/CT findings.
Both clinical and imaging findings favoured a positive
treatment response of the perineural and muscular
lymphomatous involvement in this patient with recurrent
lymphoma.
Figure 4. Maximum intensity
projection of fluorine-18
fluorodeoxyglucose positron
emission tomography/computed
tomography with significant
metabolic improvements or
resolutions of the oropharynx,
right neck and right lower
limb hypermetabolic lesions
after treated with R-IMVP-16
(rituximab, ifosfamide,
methotrexate, etoposide, and
prednisone) chemotherapy.
DISCUSSION
Perineural and muscular involvement in DLBCL is
rare, with only a limited number of cases reported in
the literature.[1] The underlying mechanisms are not fully understood, but it is believed that DLBCL may infiltrate
muscle tissue either via a haematogenous route or through
adjacent lymphatic structures.[2] Clinical manifestations
can vary widely, with patients presenting with muscle
weakness, myalgia, or neuropathic symptoms.[3]
Differential diagnoses for FDG-avid perineural and
muscular lesions include polyneuritis, compartment-related
compression radiculopathy, and tuberculosis.
In polyneuritis, the pattern of increased FDG uptake is
usually symmetrical and occurs without associated soft
tissue thickening.[4] [5] The significant soft tissue thickening
in our case made compartment-related compression
radiculopathy less likely. Active tuberculosis was
excluded through microbiological investigations.
This case demonstrated that the patient’s neuropathic
symptoms and imaging findings were indicative of
perineural and muscular involvement. The identification
of hypermetabolic activity in the muscles on 18F-FDG
PET/CT was crucial in establishing the diagnosis due to
the asymmetrical metabolic distribution and soft tissue
thickening in the affected regions. These abnormalities
resolved in parallel with the biopsy-proven recurrent
right oropharynx DLBCL, both metabolically and
morphologically. Such findings are often mistaken for
primary myopathies or neuropathies.
In our case, 18F-FDG PET/CT not only confirmed the
recurrence of DLBCL but also revealed the unusual sites
of perineural and muscular involvement. This underscores
the importance of considering extranodal manifestations
of DLBCL, as it ultimately guided treatment decisions.
Furthermore, the most recent 18F-FDG PET/CT
showed both metabolic and morphological resolution
of the hypermetabolic perineural and muscular lesions,
supporting the diagnosis of atypical lymphomatous
involvement and reflecting a significant treatment
response.
Previous studies[6] [7] revealed that perineural and muscular
involvement in DLBCL is largely underreported,
with only a limited number of cases documented—primarily in patients with advanced-stage disease—and
highlighted the importance of recognising 18F‑FDG
PET/CT findings in atypical sites of lymphomatous
involvement to avoid misdiagnosis and ensure
appropriate management. Primary muscular lymphoma[6]
and other atypical sites of DLBCL involvement[6] [7] have
also been reported.
The utility of 18F-FDG PET/CT in the staging and treatment monitoring of DLBCL has been examined,[8] [9]
which concluded that this imaging modality provides
valuable insights into disease burden and can identify sites
of active disease that may not be evident on conventional
imaging. This aligns with our case, in which 18F-FDG
PET/CT played a pivotal role in diagnosing perineural
and muscular involvement in a one-stop-shop manner.
The management of DLBCL with perineural and
muscular involvement is complex and often requires
a multidisciplinary approach.[10] [11] Treatment options
may include chemotherapy, radiotherapy, and targeted
therapies, depending on the extent of disease and the
patient’s overall health.
In our case, the patient was commenced on a salvage
chemotherapy regimen following relapse of DLBCL.
Given the aggressive nature of her disease, close
monitoring with repeat 18F-FDG PET/CT was planned
to assess treatment response. The prognosis for patients
with perineural and muscular involvement in DLBCL
varies, but early detection and timely intervention can
significantly improve clinical outcomes.
CONCLUSION
This case highlights the importance of 18F-FDG PET/CT in detecting perineural and muscular involvement in
patients with recurrent DLBCL. Early detection of the
disease involvement using 18F-FDG PET/CT can guide
biopsy targeting, inform appropriate treatment strategies
and serve as a reference for assessing treatment response
on end-of-treatment imaging, all of which are crucial for
improving patient outcomes.
REFERENCES
1. Lim AT, Clucas D, Khoo C, Parameswaran BK, Lau E.
Neurolymphomatosis: MRI and (18) FDG-PET features. J Med
Imaging Radiat Oncol. 2016;60:92-5
Crossref
2. Murthy NK, Amrami KK, Broski SM, Johnston PB, Spinner RJ.
Perineural spread of peripheral neurolymphomatosis to the cauda
equina. J Neurosurg Spine. 2021;36:464-9.
Crossref
3. Broski SM, Bou-Assaly W, Gross MD, Fig LM. Diffuse skeletal
muscle F-18 fluorodeoxyglucose uptake in advanced primary
muscle non-Hodgkin’s lymphoma. Clin Nucl Med. 2009;34:251-3.
Crossref
4. Xie X, Cheng B, Han X, Liu B. Findings of multiple neuritis on
FDG PET/CT imaging. Clin Nucl Med. 2013;38:67-9. Crossref
5. Ankrah AO, Glaudemans AW, Maes A, Van de Wiele C,
Dierckx RA, Vorster M, et al. Tuberculosis. Semin Nucl Med.
2018;48:108-30.
Crossref
6. Iioka F, Tanabe H, Honjo G, Misaki T, Ohno H. Resolution of
bone, cutaneous, and muscular involvement after haploidentical
hematopoietic stem cell transplantation followed by post-transplant
cyclophosphamide in adult T-cell leukemia/lymphoma. Clin Case
Rep. 2020;8:1553-9.
Crossref
7. Belmonte G, Caldarella C, Hohaus S, Manfredi R, Minordi LM. Muscle recurrence of a primarily nodal follicular lymphoma
studied by contrast-enhanced 18F-FDG PET/CT. Clin Nucl Med.
2020;45:65-7.
Crossref
8. Kostakoglu L, Cheson BD. Current role of FDG PET/CT in
lymphoma. Eur J Nucl Med Mol Imaging. 2014;41:1004-27.
Crossref
9. Jing F, Liu Y, Zhao X, Wang N, Dai M, Chen X, et al. Baseline
18F-FDG PET/CT radiomics for prognosis prediction in diffuse large B cell lymphoma. EJNMMI Res. 2023;13:92.
Crossref
10. Adams HJ, Kwee TC. Prognostic value of interim FDG-PET in
R-CHOP-treated diffuse large B-cell lymphoma: systematic review
and meta-analysis. Crit Rev Oncol Hematol. 2016;106:55-63.
Crossref
11. Wai SH, Lee ST, Cliff ER, Bei M, Lee J, Hawkes EA, et al. Utility
of FDG-PET in predicting the histology of relapsed or refractory
lymphoma. Blood Adv. 2024;8:736-45.
Crossref